FGF-23 in chronic kidney disease
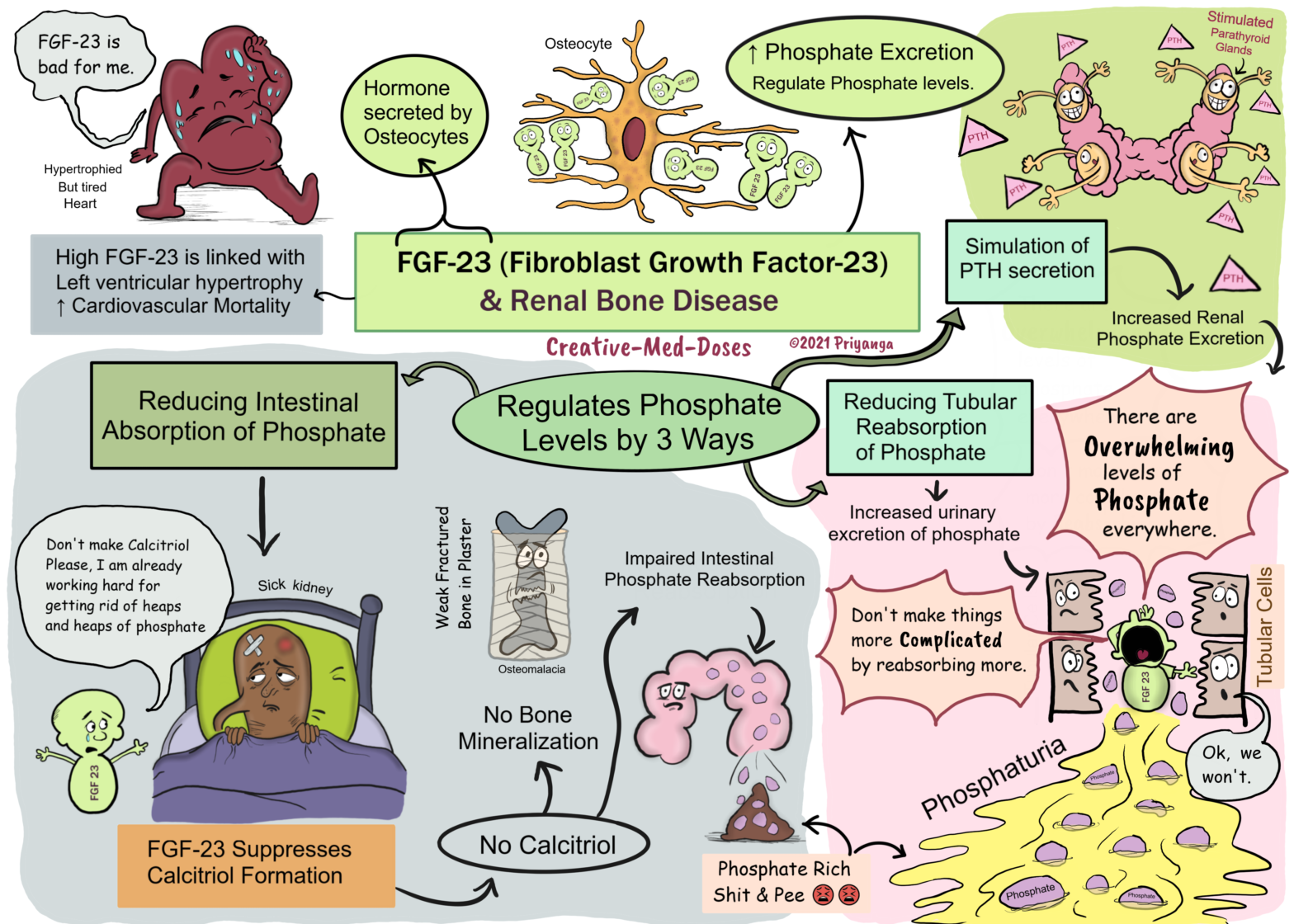
FGF-23 (fibroblast growth factor-23) is a part of a family of phosphatonins that promotes renal phosphate excretion. It is a hormone secreted by osteocytes, and it regulates phosphorus and vitamin D metabolism. FGF23 promotes phosphaturia and decreases the production of calcitriol.
Its levels increase in early CKD as a physiological adaptation to maintain normal serum phosphate levels.
FGF-23 maintains normal serum phosphorus levels by three mechanisms:
(1) Phosphaturia- Increased renal phosphate excretion (by reducing tubular reabsorption of phosphorus)
(2) Secondary Hyperparathyroidism- stimulation of PTH, which also increases renal phosphate excretion
(3) Suppresses calcitriol formation– suppression of the formation of 1,25(OH)2 D3, leading to diminished phosphorus absorption from the GI tract.
It becomes maladaptive by causing a progressive decline in 1,25(OH)(2)D levels. It leads to secondary hyperparathyroidism and related complications of bone metabolism.
Post Type Archives: Topics
Hypothalamic-Pituitary-Ovarian axis
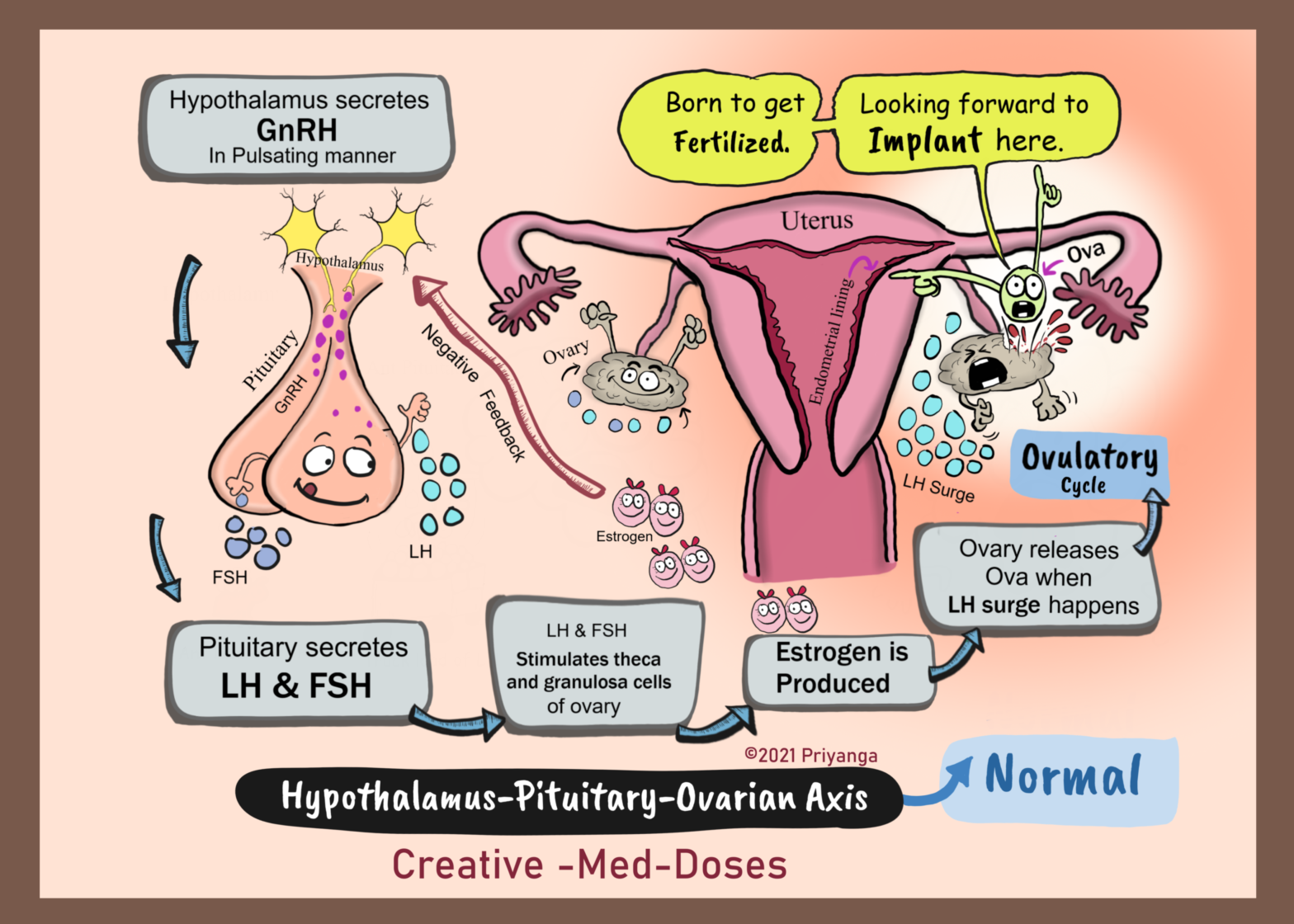
Hypothalamic-pituitary-ovarian (HPO) axis has three components –
Hypothalamus – It is located at the base of the brain, above the brainstem. It secretes gonadotropin-releasing hormone (GnRH).
Pituitary – it is located in the base of the skull just below the hypothalamus, and pulsatile release of GnRH from the hypothalamus stimulates the secretion of Follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
Ovaries- FSH and LH from the pituitary stimulates granulosa cells and theca cells of the ovaries to secrete estrogen and progesterone. Excess in estrogen causes negative feedback and causes inhibition of GnRH release from the hypothalamus.
FSH stimulates primordial follicles to mature by acting on granulosa cells, the fall in FSH causes the selection of dominant follicles. The follicles which have the highest number of FSH receptors get more concentrated FSH micro-environment and thus they grow faster and become dominant follicle one of these dominant follicles releases ova every month. Only one of the maturing follicles can dominate over the others. It is called the Graafian follicle.
The Granulosa cells of these follicles produce estrogen which stimulates the hypothalamus to secrete GnRH. There is LH and FSH surge 24 hours before ovulation, this surge causes Graafian follicle to release ova. This phase of the reproductive cycle, from FHS release until ovulation, is called the follicular phase.
After ovulation, the ruptured follicle becomes the corpus luteum. In addition to producing estrogen, it also produces progesterone. Progesterone stimulates the uterine endometrium’s secretory functions and signals the hypothalamus to stop producing GnRH. This, in turn, deactivates FSH and LH production.
Congenital Solitary Kidney
Congenital Solitary Kidney introduction slide
Congenital Solitary Kidney is a congenital anomaly where the affected person has only one functioning kidney. It can be due to the absence or anomaly of the contralateral kidney.
Causes
Anatomical – in these cases, the person has only a single kidney since birth. Unilateral Renal agenesis
Functional- in these cases, the person has two kidneys, but only one kidney is functional. Renal aplasia, hypoplasia, or dysplasia can lead to such situations.
Compensatory renal hypertrophy develops in solitary kidneys. In most cases, it remains asymptomatic. They are diagnosed during prenatal ultrasound screening or routine examination in younger children. Recent research says that there is Hyperplasia in the solitary kidney as it has double the number of nephrons in comparison to the normal kidney.
Associated complications
The compensatory hypertrophy causes hyperfiltration →increased podocytes and, basement injury →Loss of functional renal parenchyma →Chronic kidney disease and renal insufficiency →End-stage renal disease (ESRD)
Vesicoureteral reflux
Increased risk of hypertension
Neuropathic arthropathy: Charcot arthropathy
Neuropathic arthropathy: Charcot arthropathy
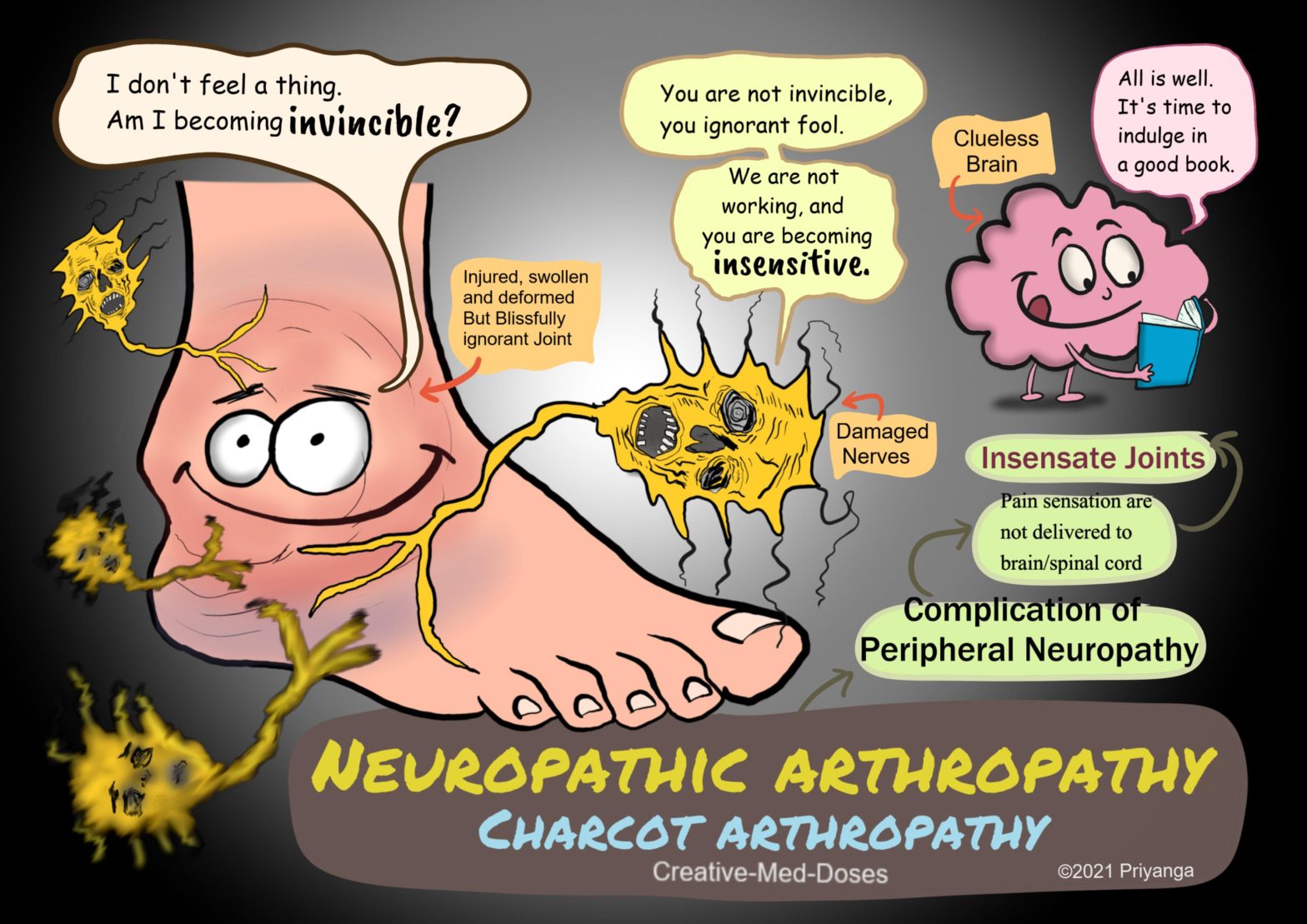
Neuropathic arthropathy (Charcot arthropathy) is a complication of peripheral neuropathy that results in fractures, dislocations, subluxations. It has an increased risk of progressive deformity of the affected joint. Sometimes, the resulting joint deformity increases the risk of amputation.
Charcot arthropathy is a specific manifestation of peripheral neuropathy, also known as Neuropathic Joint Disease. It is named after Jean-Martin Charcot, who recognized that peripheral neuropathy could lead to neuropathic joints. Any condition resulting in decreased peripheral sensation, proprioception, and fine motor control can cause Charcot arthropathy. There is a progressive degeneration of a weight-bearing joint. The affected joint has bony destruction, bone resorption, and eventual deformity.
Most common locations
• Foot and ankle (most commonly affected joint)
• Shoulder
• Elbows
Conditions causing neuropathy and Charcot arthropathy
• Diabetes mellitus- foot and ankle are most affected
• Tertiary syphilis (tabes dorsalis) – the knee is the most affected joint
• Syringomyelia – shoulder is the most affected joint
• Trauma
• Leprosy
• Spinal cord tumor
• Subacute combined degeneration (Vit B12 deficiency)
Pathophysiology (underlying mechanisms responsible for the neuropathic joint)
Mechanisms are responsible for joint destruction in these cases are-
Neurotrauma
Peripheral neuropathy → loss of sensation, proprioception, and deep tendon reflexes → imbalanced and clumsy joints with poor fine motor control → repetitive trauma → no pain since joint is insensate → patient remains unaware of injury and doesn’t fix it → prolonged inflammation, destruction and Injury continues → swollen, red and nontender joint in beginning → deformed joint later in course of the disease → may lead to amputation
Neurovascular
Repetitive injury → Joint inflammation → increased blood flow towards the joint by dilating vessels → Autonomic Neuropathy → reduced ability to vasoconstrict → vessels fails to constrict → hyperemia in injured and inflamed joint → stimulates osteoclasts → increased osteoclast-mediated bone resorption→ decreased bone mineral density→ osteopenia→ increased risk of fractures and the deformity
Clinical presentation
Acute arthropathy – patient presents with swollen, erythematous but nontender joint. Physical examination shows loss of sensation and absent deep tendon reflexes (DTR)
Chronic arthropathy- patient presents with deformed joint, bony prominences, and foot ulcers. The most common deformity is a collapse of the tarsometatarsal joint, with valgus angulation.
Analgesic Nephropathy: pain killers killing kidneys
Analgesic nephropathy is chronic tubulointerstitial nephritis. It is caused by long-term use of high doses (>1-2 Kgs) of certain analgesics, especially if taken in combinations.
The combinations of the following analgesics are most commonly associated with AN-
• phenacetin, aspirin, and caffeine
• phenacetin-acetaminophen
• NSAIDs and acetaminophen
most analgesics (including NSAIDs) reduce pain by inhibiting prostaglandin (PG) synthesis. Prostaglandins have a vasodilatory effect which helps in the maintenance of renal blood flow. In patients with normal renal function and normal volume state, the renal synthesis of PG is low, and it does not play a significant role in the maintenance of renal blood flow.
But in decreased renal perfusion, the local synthesis of vasodilator prostaglandins is increased. And renal perfusion is maintained. This autoregulatory mechanism is crucial for adequate renal blood flow: in cases with volume contracted states (congestive heart failure, ascites, hepatic failure, and chronic kidney disease, diuretic users, and the elderly with vascular damage/atherosclerosis).
Mechanism of renal injury, prostaglandin is blocked by analgesics –
Analgesics in high doses → inhibition of prostaglandin synthesis → less prostaglandin for renal vasodilation→ reduced renal blood flow → increased chances of ischemic and hypoxic injury to tubules and interstitial tissue→ acute kidney injury
Acute Tubular Necrosis/Injury
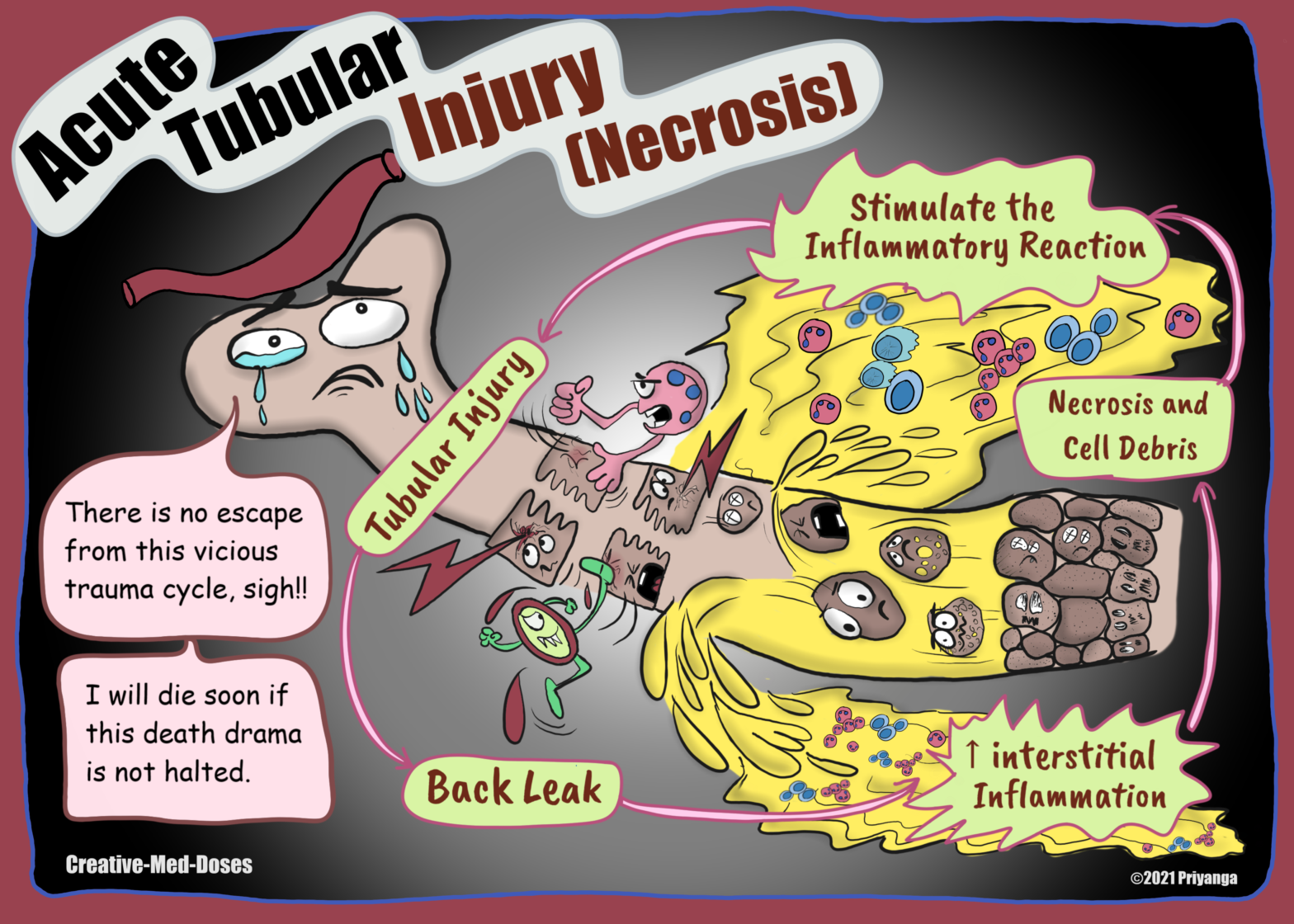
Acute tubular necrosis (ATN) is characterized by damage to tubular epithelial cells and abrupt decline in renal function. There is the shedding of granular muddy brown casts and tubular epithelial cells into the urine. ATN is the most common cause of acute kidney injury and may cause oliguria (urine output of <400 mL/day). It is the most common cause of AKI in hospitalized patients. It is associated with high morbidity and mortality.
Detrusor and Sphincters
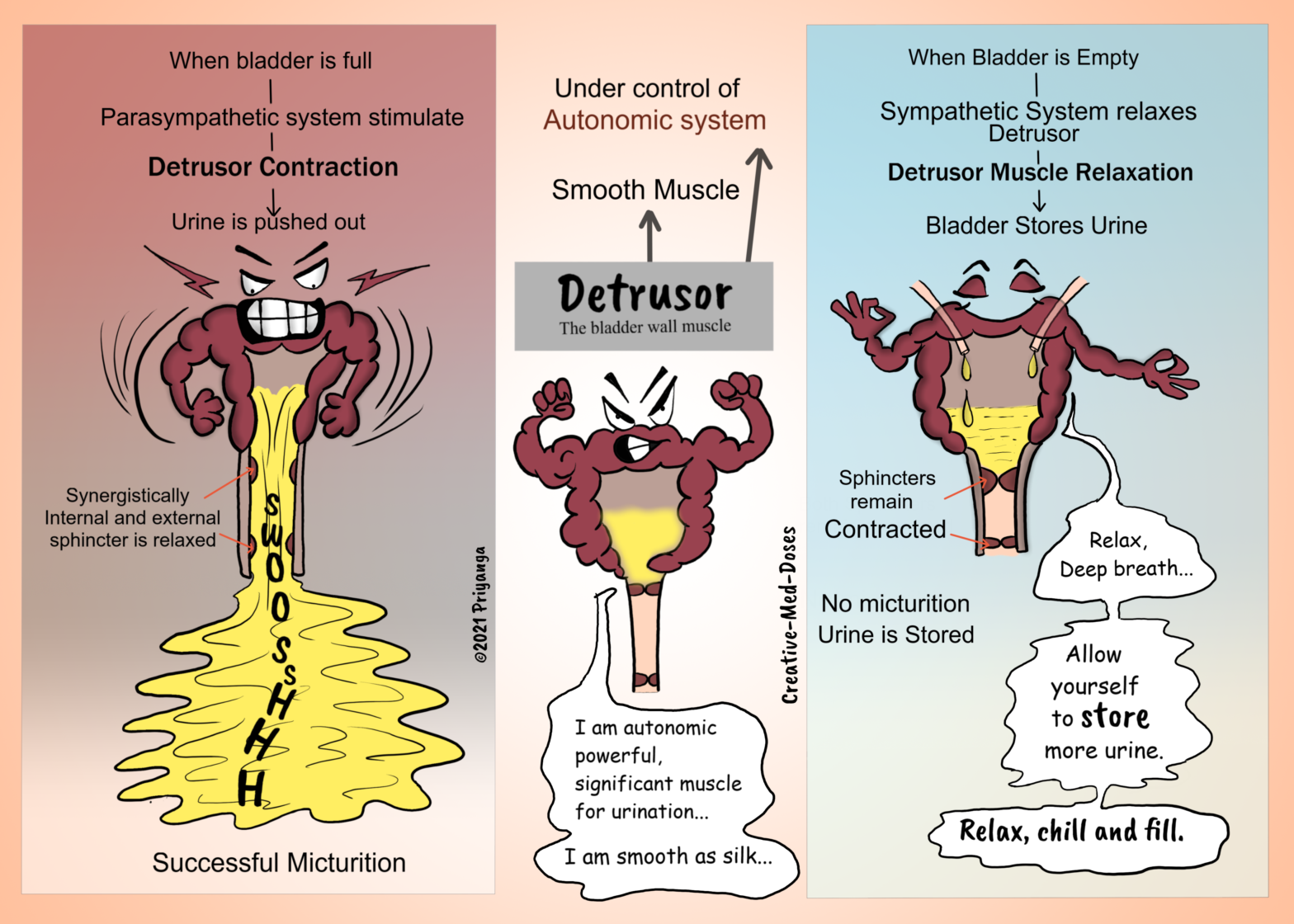
Bladder musculature has an important role in the storage and emptying of urine from the bladder.
Detrusor
The bladder wall contains specialized smooth muscle – known as detrusor muscle which contracts during micturition and pushes urine out of the bladder. The fibers of the detrusor muscle are arranged in multiple directions. It retains the structural integrity of the bladder when stretched. The detrusor receives innervation from both the sympathetic and parasympathetic nervous systems. It is under the control of the autonomic nervous system.
Spinal cord lesions and the bladder
The bladder has important clinical considerations when it comes to spinal cord lesions. There are two different clinical syndromes, depending on where the damage has occurred.
Spinal Cord Transection Above T12- Reflex Bladder
The afferent signals from the bladder wall are unable to reach the brain → no awareness of bladder filling → no descending control over the external urethral sphincter→ external urethral sphincter is constantly relaxed voluntary control over micturition is lost bladder empties as it fills (like newborn have spinal reflex and no voluntary control on micturition (like newborn babies).
In spinal reflex, the parasympathetic system initiates detrusor contraction in response to bladder wall stretch. The bladder automatically empties as it fills – known as the reflex bladder.
Spinal Cord Transection Below T12- Flaccid Bladder (detrusor areflexia)
Damaged parasympathetic outflow to the bladder → detrusor muscle is paralyzed and unable to contract → the bladder will fill uncontrollably → becomes abnormally distended until overflow incontinence occurs.
Detrusor Hypertrophy (myogenic bladder)
The fibers of the detrusor muscle often become hypertrophic (presenting as prominent trabeculae) to compensate for the increased workload of the bladder emptying, in cases of bladder outlet obstruction (for example in Benign prostatic hyperplasia). Eventually, these hypertrophic muscles will become fibrotic and rigid, making a weak noncompliant bladder wall.
Detrusor sphincter dyssynergia (DSD)
The human bladder has two functions—to store and empty urine. The Coordination and transition between these functions require synergy among the detrusor muscle, urinary sphincters, and the central nervous system. DSD is diagnosed via urodynamic studies in neurogenic bladder patients.
When the central neurologic pathways controlling urine storage and emptying are disrupted by injury, inflammation, degenerative process, or congenital malformation, the urinary sphincters and detrusor can lose coordination leading towards dyssynergia.
If the detrusor muscle contracts while the sphincter is contracted, there is functional bladder outlet obstruction. Detrusor sphincter dyssynergia (DSD) is the urodynamic description of this neurologically induced bladder outlet obstruction.
Hydronephrosis: Dilated Pelvis and calyx
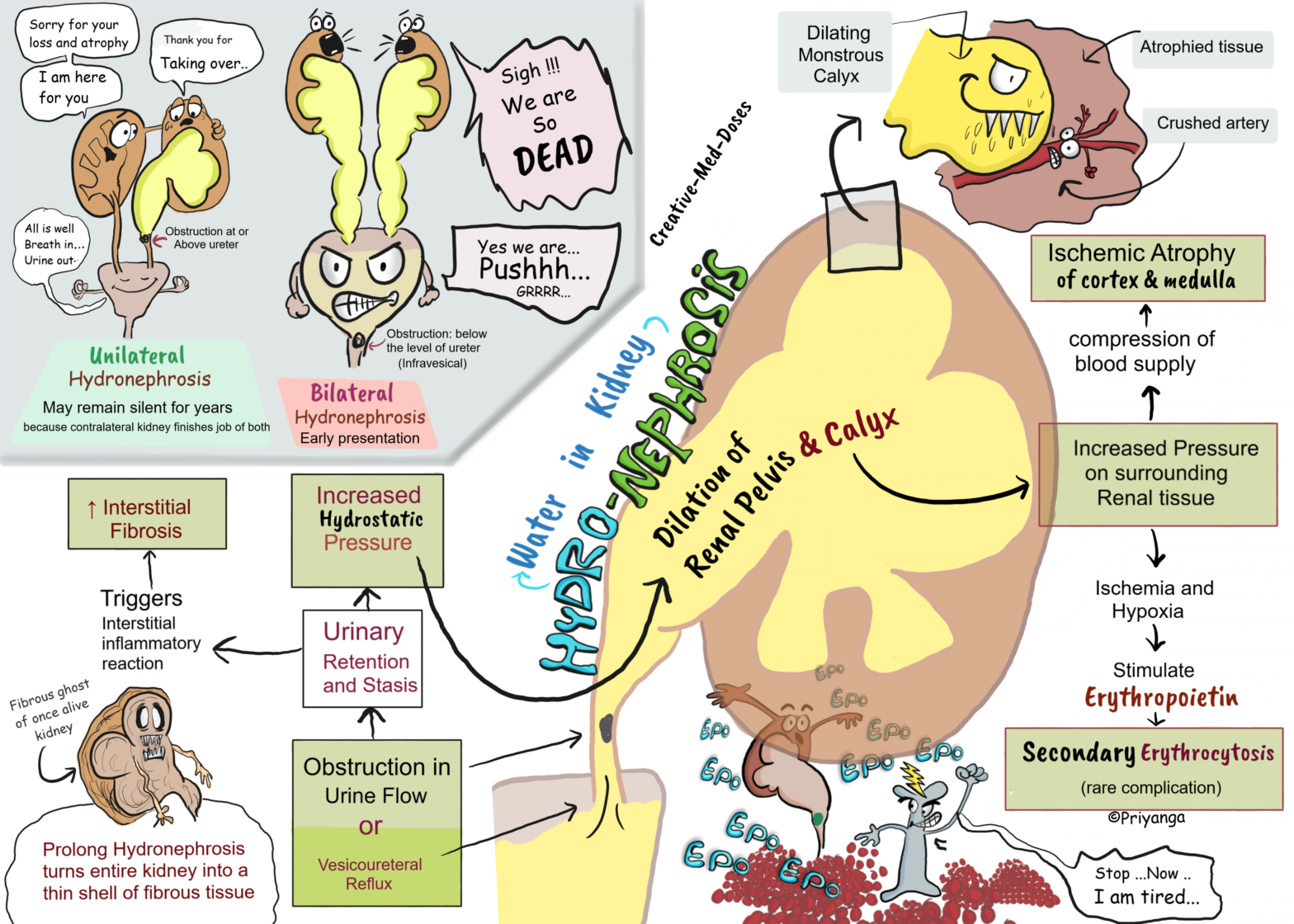
Hydronephrosis means dilation of renal calyx and pelvis. It occurs due to an obstruction in urine flow or vesicoureteral reflux leading towards urinary retention and stasis. The urinary tract obstruction may be sudden or insidious.
Lower urinary tract obstruction: clinical features
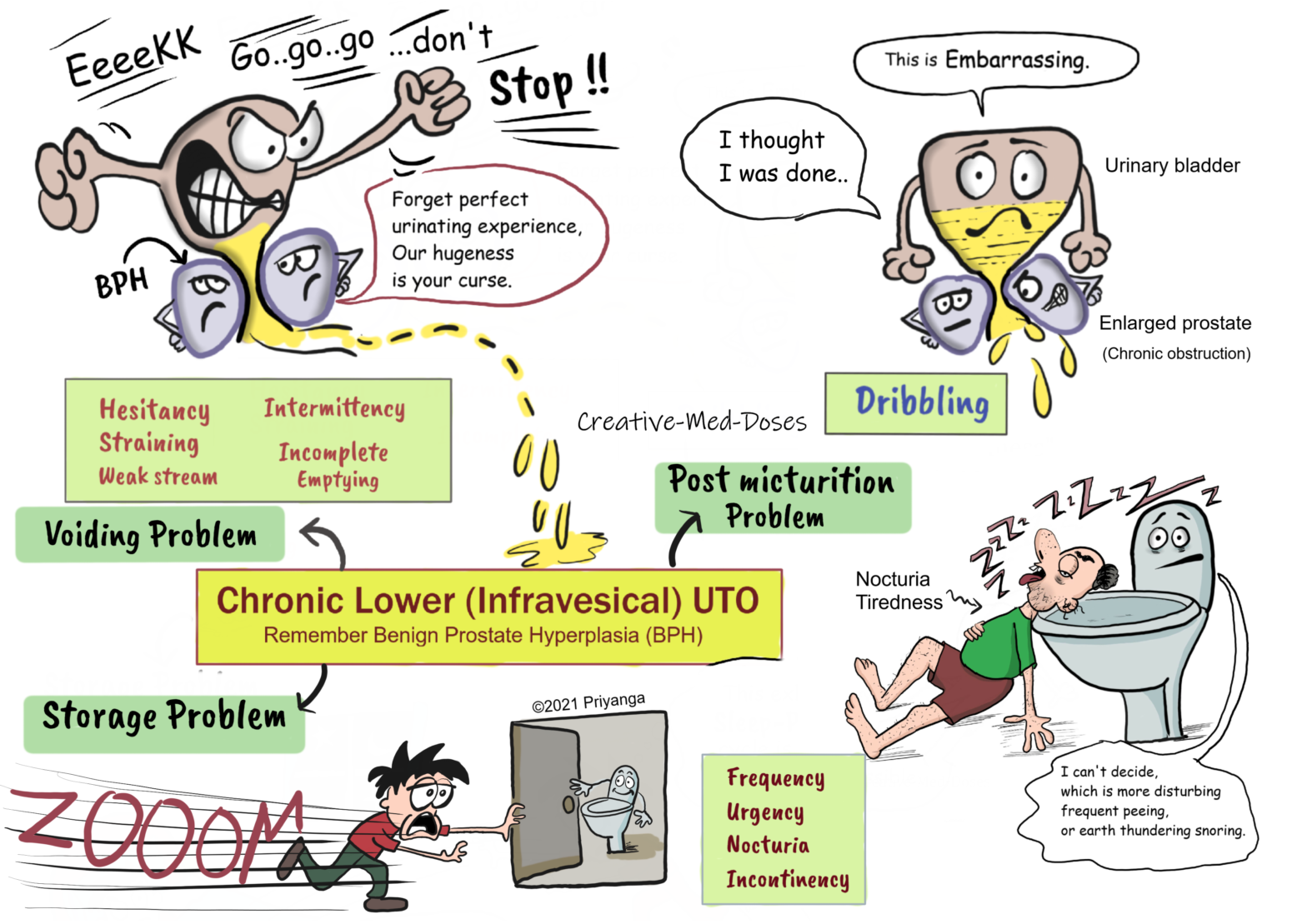
Lower urinary tract (infravesical) obstruction can be acute or chronic. The clinical features depend upon duration, etiology, and site of the obstruction
Acute obstruction
Acute obstruction is an emergency, and obstruction should be relieved as early as possible, remember stone lodged at the bladder neck.
Urinary retention- acute blockage causes impaired urine flow and urinary stasis. It increases hydrostatic pressure in the urinary bladder.
Suprapubic pain- due to urinary retention and stretching of the bladder, it is excruciating pain.
Palpable bladder- the distended bladder is palpated near the lower abdomen (suprapubic area).
Friedreich’s ataxia: absent frataxin
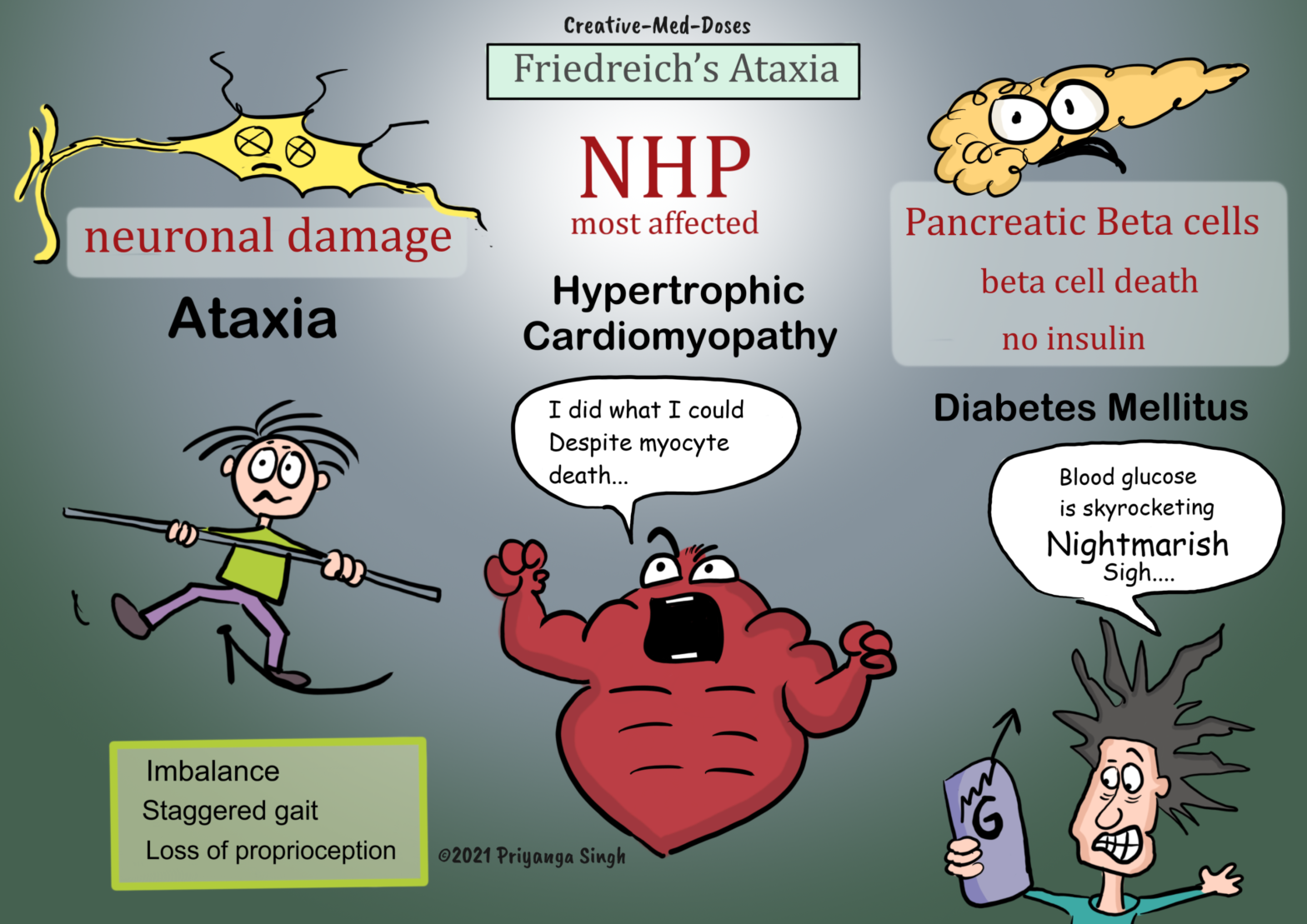
Friedreich’s ataxia is the most common form of inherited ataxia. It has congenital impairment of mitochondrial function leading to cerebellar and spinal cord atrophy and neurodegeneration.