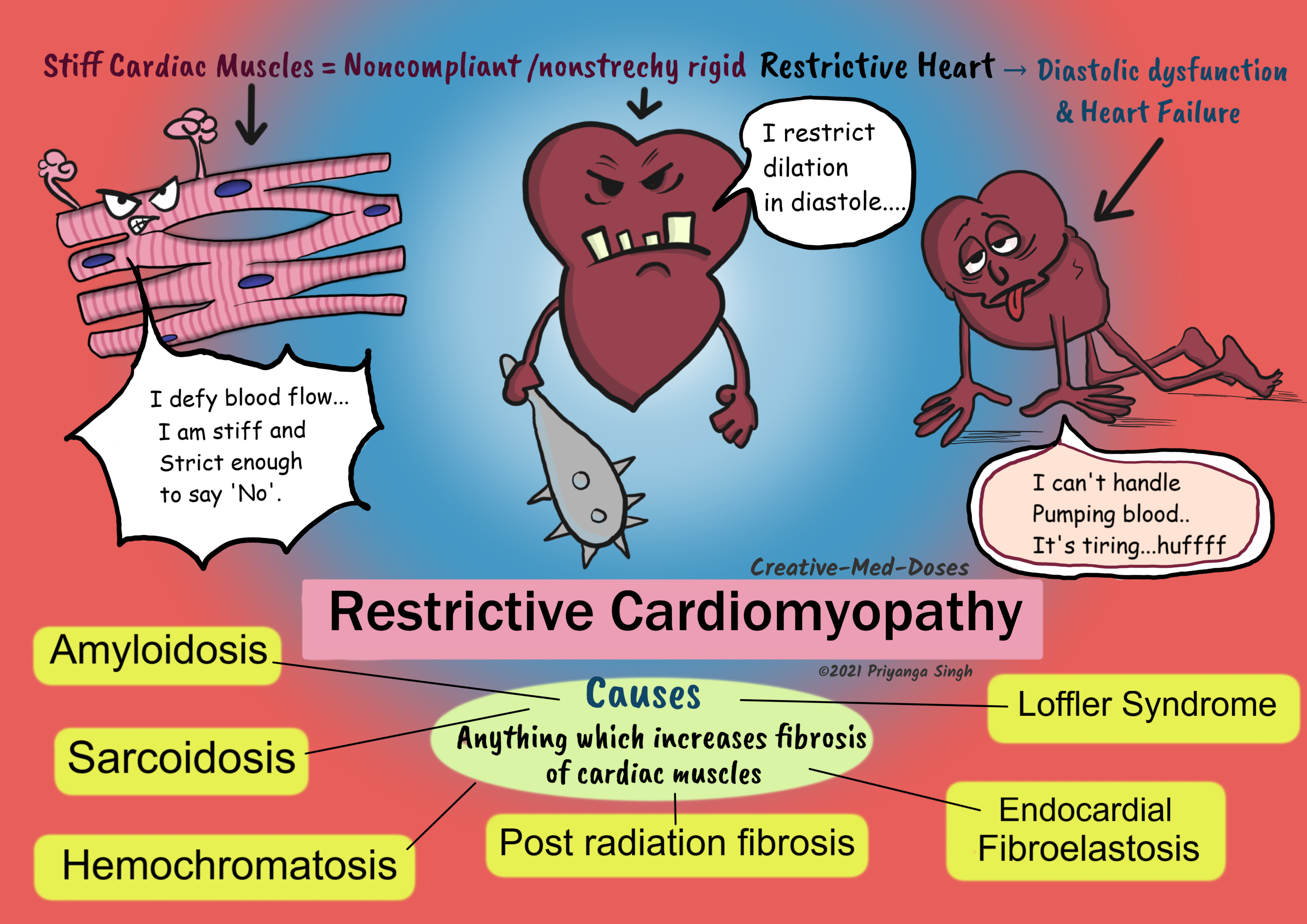
Restrictive Cardiomyopathy: Stiff Ventricles
Restrictive cardiomyopathy is a primary disease of ventricular compliance. It causes impaired ventricular filling during diastole because the ventricular wall is stiffer and noncompliant.
Causes
- Idiopathic
- Amyloidosis- deposition of insoluble β-pleated sheets causes stiff ventricular muscles. Some immunoglobulin light chains are directly cardiotoxic and can induce myocardial dysfunction.
- Hemochromatosis- iron deposition can induce free radicle injury and fibrosis of cardiac muscles. It is most commonly associated with dilated cardiomyopathy but can also cause restrictive cardiomyopathy.
- Sarcoidosis – granuloma formation, and chronic inflammatory reaction in cardiac muscles cause fibrosis and stiffening of heart muscles
- Scleroderma
- Post radiation fibrosis – radiation exposure is associated with free radicle formation and fibrosis.
- Loffler Syndrome- It has peripheral hyper-eosinophilia, and eosinophilic tissue infiltrates. The release of eosinophil granule contents causes endocardial and myocardial necrosis. It causes the scarring, and layering of the endocardium by thrombus. The thrombus organization leads to stiffened and noncompliant ventricles.
- Endomyocardial Fibrosis- there is dense diffuse fibrosis of the ventricular endocardium and subendocardium. It involves the tricuspid and mitral valves. The fibrous tissue markedly diminishes the volume and compliance. Endomyocardial fibrosis is associated with nutritional deficiencies and inflammation related to helminthic infections.
- Malignancy
Pathogenesis
Stiff and rigid noncompliant myocardium → impaired ventricular filling → diastolic dysfunction gradual reduction in ejection fraction → heart failure (right-sided is more common)
Clinical presentation mimics constrictive pericarditis.
Morphology
The ventricles are of approximately normal size or only slightly enlarged and, the cavities are not dilated.
Both atria are typically dilated as a consequence of restricted ventricular filling and pressure overloads.
Microscopic examination shows interstitial fibrosis and, deposition of various substances. The biopsy has the main role in confirming the diagnosis and etiology of restrictive cardiomyopathy.
...
...
Clinical presentation
The patient rarely presents with exercise intolerance and dyspnea which are earlier symptoms. Most cases present as a congestive failure and right-sided failure dominates the clinical picture. Read more on heart failure Heart Failure: Left sided VS Right sided - Creative Med Doses
- Edema
- Congestive Hepatomegaly
- Ascites
- Jugular venous distention
- Kussmaul sign (read more here Kussmaul Sign and inspiration - Creative Med Doses)
Diagnosis
Based on clinical presentation, echocardiogram, and biopsy
ECG (electrocardiogram) – Shows low voltage
Endomyocardial biopsy – it is the most accurate diagnostic test to determine etiology of Restrictive cardiomyopathy. Especially, amyloidosis where apple-green birefringence is noticed on Congo stain. And Loffler syndrome where eosinophilic infiltrates are seen.
Treatment
Management of symptoms and treatment of underlying etiology is the goal.
A heart transplant is definitive treatment.
Diuretics – to reduce fluid overload in congestive failure
Phlebotomy in cases of hemochromatosis
Buy fun review books here (these are kindle eBook’s you can download kindle on any digital device and login with Amazon accounts to read them). Have fun and please leave review.
https://creativemeddoses.com/books/