Detrusor and Sphincters
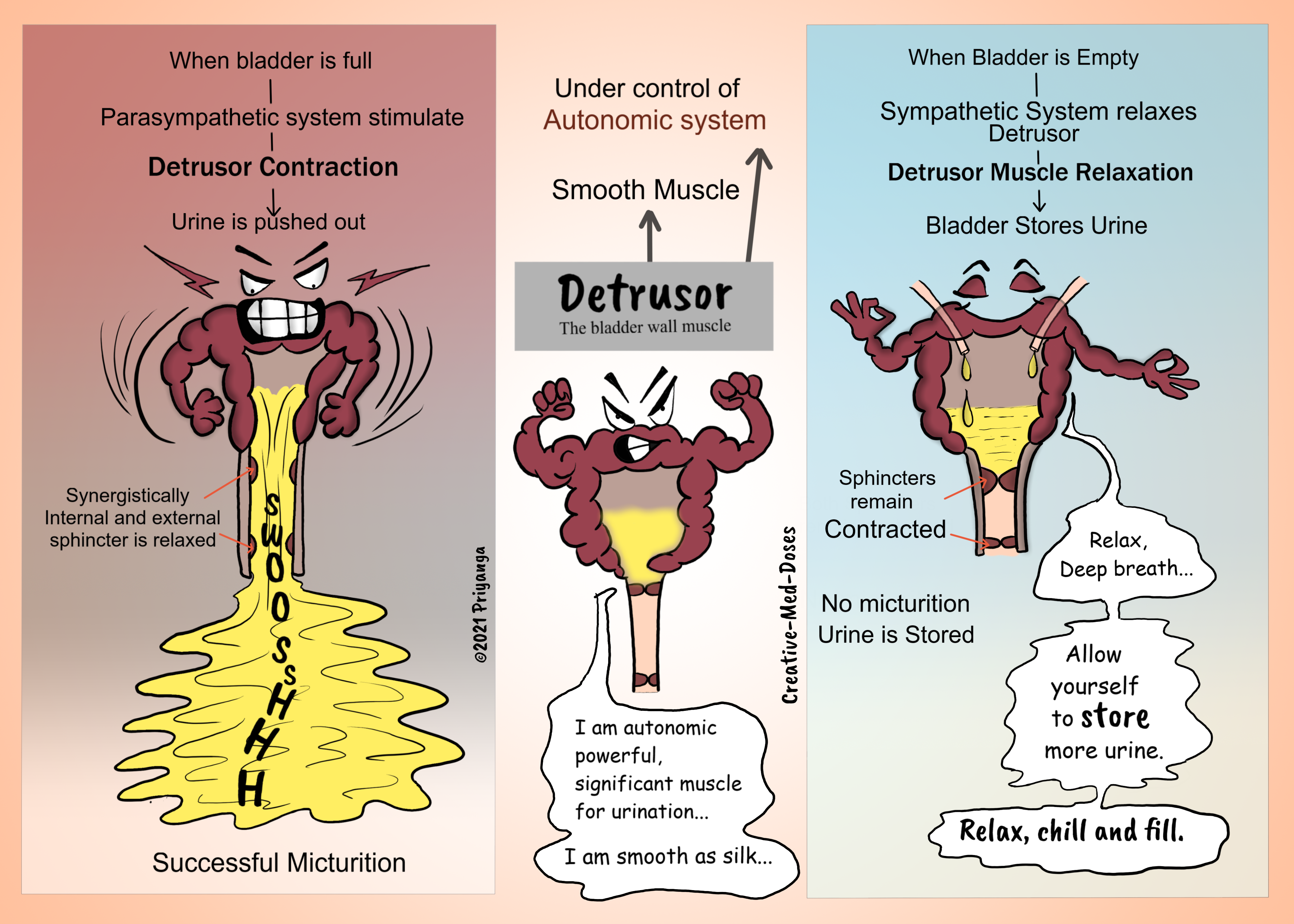
Detrusor has an important role in the storage and emptying of urine from the bladder. It is a specialized smooth muscle that forms the bladder wall. The fibers of the detrusor muscle are arranged in multiple directions. It retains the structural integrity of the bladder when stretched. The detrusor receives innervation from both the sympathetic and parasympathetic nervous systems. It is under the control of the autonomic nervous system.
Bladder musculature has an important role in the storage and emptying of urine from the bladder.
The urethra has two muscular sphincters:
- Internal urethral sphincter:
In Male, it consists of circular, smooth fibers, which are under autonomic control. It also prevents seminal regurgitation during ejaculation.
In Females, it is a functional sphincter (there is no sphincteric muscle present as such). The anatomy of the bladder neck and the proximal urethra forms a functional internal sphincter.
- External urethral sphincter – has the same structure in both sexes. It is skeletal muscle and under voluntary control (pudendal nerve).
Nervous Supply
The bladder receives input from both the autonomic (sympathetic and parasympathetic) and somatic parts of the nervous system. The coordination between the nervous system and bladder muscles is important for the smooth functioning of the bladder.
The sympathetic – hypogastric nerve (T12 – L2), causes relaxation of the detrusor muscle, promoting urine storage.
The Parasympathetic – pelvic nerve (S2-S4) and Increased signals from this nerve cause contraction of the detrusor muscle, stimulating micturition.
The Somatic- Pudendal nerve (S2-4). It innervates the external urethral sphincter, providing voluntary control over micturition.
Sensory (afferent) nerves- reports to the brain and spinal cord. They are found in the bladder wall (stretch receptors) and signal the need to urinate when the bladder becomes full.
The human bladder has two functions—to store and empty urine. The coordination and transition between these functions require synergy among the detrusor muscle, urinary sphincters, and the nervous system. Disruption and dysfunction at any level can affect urine storage and micturition.
The Bladder Stretch Reflex
The bladder stretch reflex is a primitive spinal reflex. The micturition is stimulated in response to the stretch of the bladder wall. It is analogous to a muscle spinal reflex, such as the patella reflex.
The reflex arc:
- The bladder fills with urine, and the bladder walls stretch. Sensory nerves detect stretch and transmit this information to the spinal cord.
- Interneurons within the spinal cord relay the signal to the parasympathetic efferents (the pelvic nerve).
- The pelvic nerve acts to contract the detrusor muscle and stimulate micturition.
Although it is non-functional post-childhood, the bladder stretch reflex needs to be considered in spinal injuries (where the descending inhibition cannot reach the bladder), and in neurodegenerative diseases (where the brain is unable to generate inhibition).
...
...
Clinical Relevance
Spinal cord lesions and the bladder
The bladder has important clinical considerations when it comes to spinal cord lesions. There are two different clinical syndromes, depending on where the damage has occurred.
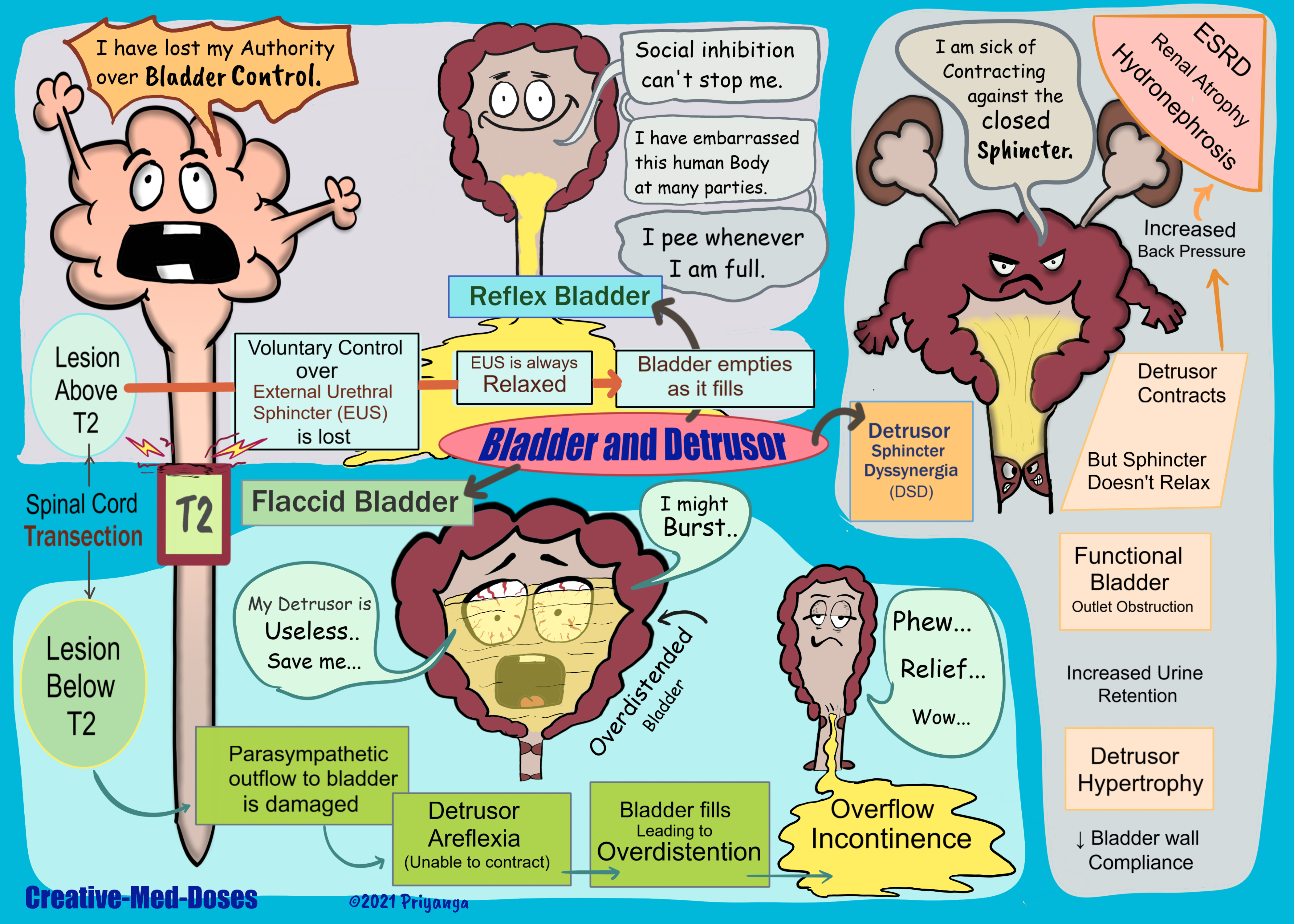
Spinal Cord Transection Above T12- Reflex Bladder
The afferent signals from the bladder wall are unable to reach the brain → no awareness of bladder filling → no descending control over the external urethral sphincter→ external urethral sphincter is constantly relaxed voluntary control over micturition is lost bladder empties as it fills (like newborn have spinal reflex and no voluntary control on micturition (like newborn babies).
In spinal reflex, the parasympathetic system initiates detrusor contraction in response to bladder wall stretch. The bladder automatically empties as it fills – known as the reflex bladder.
Spinal Cord Transection Below T12- Flaccid Bladder (detrusor areflexia)
Damaged parasympathetic outflow to the bladder → detrusor muscle is paralyzed and unable to contract → the bladder will fill uncontrollably → becomes abnormally distended until overflow incontinence occurs.
Detrusor Hypertrophy (myogenic bladder)
The fibers of the detrusor muscle often become hypertrophic (presenting as prominent trabeculae) to compensate for the increased workload of the bladder emptying, in cases of bladder outlet obstruction (for example in Benign prostatic hyperplasia). Eventually, these hypertrophic muscles will become fibrotic and rigid, making a weak noncompliant bladder wall.
Detrusor sphincter dyssynergia (DSD)
The human bladder has two functions—to store and empty urine. The Coordination and transition between these functions require synergy among the detrusor muscle, urinary sphincters, and the central nervous system. DSD is diagnosed via urodynamic studies in neurogenic bladder patients.
When the central neurologic pathways controlling urine storage and emptying are disrupted by injury, inflammation, degenerative process, or congenital malformation, the urinary sphincters and detrusor can lose coordination leading towards dyssynergia.
If the detrusor muscle contracts while the sphincter is contracted, there is functional bladder outlet obstruction. Detrusor sphincter dyssynergia (DSD) is the urodynamic description of this neurologically induced bladder outlet obstruction.
The timely diagnosis of DSD is important because the condition has the potential to cause renal failure. When the detrusor contracts against the closed sphincter, there is sustained bladder storage pressure.
If the pressure in the bladder remains higher for a longer time, it will cause increased hydrostatic pressure (back pressure) in the upper urinary tract. It leads to vesicoureteral reflux and dilatation of the upper urinary tract (hydronephrosis and hydroureter). Increased urinary retention also causes recurrent urinary tract infections and renal stones. Chronic hydronephrosis causes renal atrophy and ESRD.
Undiagnosed and untreated DSD has a higher risk of loss of bladder compliance, hydronephrosis and consequently causes renal compromise and end-stage renal disease (ESRD).
...
...
Treatment for DSD-
Intermittent catheterization combined with anticholinergics- It reduces bladder pressure (detrusor pressure) and increases bladder compliance. It is the most common treatment for DSD.
Surgical sphincterotomy
Pharmacologic sphincterotomy- The periurethral injections of botulinum toxins inhibit acetylcholine release from cholinergic nerve terminals. It inhibits striated and smooth muscle contractions.
Urethral overdilation through the balloon improves bladder compliance and reduces outlet resistance.
Urethral stent - Urethral stents are a controversial treatment option for managing DSD in the neurogenic bladder patient. In this surgeon place a rigid, non-compressible material across the dysfunctional external sphincter to maintain urethral patency.
Malignancy and Detrusor
Bladder cancer invading detrusor is considered a T2 lesion. Muscle invasive bladder cancer has a different mode of treatment than cancer confined to the submucosa. In most cases with muscle-invasive bladder cancer, radical cystectomy is the treatment of choice. So, it is crucial to detect muscle invasion before starting therapy for bladder cancer.
Revision for today Hydronephrosis: Dilated Pelvis and calyx - Creative Med Doses
Buy fun review books here (these are kindle eBook’s you can download kindle on any digital device and login with Amazon accounts to read them). Have fun and please leave review.
https://creativemeddoses.com/books/