Acute Tubular Necrosis/Injury
Acute tubular necrosis (ATN) is characterized by damage to tubular epithelial cells and abrupt decline in renal function. There is the shedding of granular muddy brown casts and tubular epithelial cells into the urine. ATN is the most common cause of acute kidney injury and may cause oliguria (urine output of <400 mL/day). It is the most common cause of AKI in hospitalized patients. It is associated with high morbidity and mortality.
The term tubular necrosis is a misnomer, as cellular necrosis is usually minimal. Acute tubular injury is a frequently used term by pathologists to describe this lesion.
Etiology
Acute tubular necrosis happens due to sudden ischemic or toxic events or sepsis.
Ischemic-
Anything causing reduced renal perfusion-
Prerenal azotemia and ischemic acute tubular necrosis have the same spectrum of causes. Any factor that leads to prerenal azotemia can lead to ischemic acute tubular necrosis.
- severe trauma
- blood loss
- acute pancreatitis
- septicemia
- microscopic polyangiitis
- malignant hypertension
- thrombotic microangiopathies
- mismatched blood transfusions and other hemolytic crises (hemoglobinuria)
- myoglobinuria (crush syndrome)
Nephrotoxic substances
- Heavy metals – mercury and lead poisoning
- Organic solvents- carbon tetrachloride
- Drugs- Gentamycin, cisplatin
- Radiographic contrast agents
- Crush injury (myoglobinuria)
- Hemoglobinuria (hemolytic anemia)
Pathogenesis
Decreased glomerular filtration rate (GFR) is associated with acute tubular necrosis. There are three mechanisms of injury to the renal tubular epithelial cells-
- Renal vasoconstriction -Afferent arteriolar vasoconstriction in response to tubulo-glomerular feedback (RAAS activation, increased endothelin). Ischemia leads to decreased production of vasodilators ( nitric oxide, prostacyclin) by the tubular epithelial cells. It leads to further vasoconstriction and hypoperfusion.
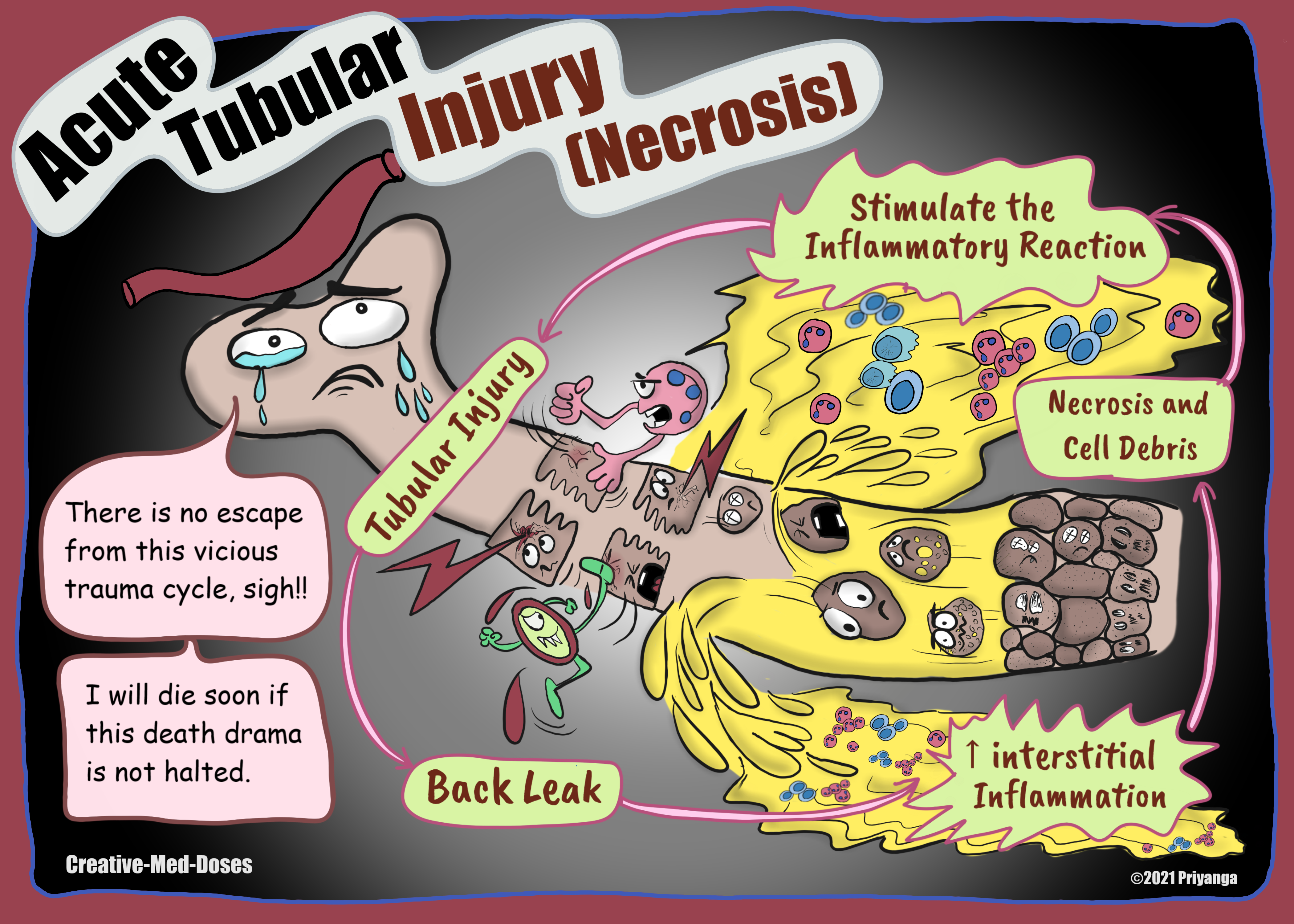
- Back-leak of glomerular filtrate from the injured tubular wall
- Tubular obstruction by debris and cast
Acute tubular necrosis is divided into three phases-
Initiation phase
The ischemia or nephrotoxin causes tubular injury, and hypoxia and tubular damage and dysfunctions begin.
Proximal tubular epithelial cells and thick loop of Henle are sensitive to hypoxemia and nephrotoxins. Following are the main reason hypothesized behind their vulnerability -
PCT and Loop of Henle dip into the relatively hypoxic medulla.
Proximal tubule and thick loop of Henle have elevated intracellular concentration of various molecules. These molecules are reabsorbed or secreted across the tubular epithelial cells. The energy required for reabsorption and secretion comes from ATP. The ATP generation needs oxygen. That's why PCT and the Thick loop of Henle have a high rate of oxygen consumption and are vulnerable to oxygen-deprived states like ischemia.
Ischemia causes multiple structural alterations in tubular epithelial cells.
- Loss of cell polarity
- Attenuation of tubular brush borders
- Blebbing and sloughing of brush borders
- Vacuolization of cells
- Detachment of tubular cells from their underlying basement membranes with sloughing of cells into the urine
This sloughed pile of debris obstructs the tubular lumen and causes obstruction in urine flow and oliguria or anuria.
The filtration fluid accumulation causes increased intratubular pressure and reduced filtration pressure gradient. It exacerbates the decline in GFR.
Also, the fluid from the damaged tubules leaks back into the interstitium, resulting in decreased urine output, increased interstitial pressure, and collapse of the tubules. Tubular collapse contributes to worsening oliguria and decline in GFR.
Necrotic tubular cells may stimulate an inflammatory reaction that contributes to tubular injury and functional derangements.
The ischemia and nephrotoxins stimulate intrarenal vasoconstriction. Ischemia results in reduced glomerular plasma flow and reduced oxygen delivery to the tubules in the outer medulla (thick ascending limb and straight segment of the proximal tubule).
Increased release of the endothelial vasoconstrictor endothelin and decreased vasodilatory nitric oxide and prostaglandins contributes to renal vasoconstriction in tubular injury.
...
...
Maintenance phase
The GFR is at a very low level (oliguric phase), and it generally lasts 1-2 weeks. Uremic complications, metabolic abnormalities, and electrolyte imbalance predominate. Metabolic acidosis and hyperkalemia are the most commonly seen electrolyte imbalance.
Recovery phase
The recovery phase (Polyuric phase) is characterized by the regeneration and repair of tubular epithelial cells. During recovery, diuresis causing salt and water loss and volume depletion might occur. The diuresis is due to the delayed recovery of tubular cell function in the setting of increased glomerular filtration (GFR comes to normal first, and tubular reabsorption is legging in recovery. BUN and Creatinine levels return to normal, and there is a risk of hypokalemia in this stage.
Revision for today Hydronephrosis: Dilated Pelvis and calyx - Creative Med Doses
Buy fun review books here (these are kindle eBook’s you can download kindle on any digital device and login with Amazon accounts to read them). Have fun and please leave review.