ZOLLINGER–ELLISON SYNDROME: ZES
ZOLLINGER–ELLISON SYNDROME (ZES) Severe peptic ulcer diathesis secondary to gastric acid hypersecretion due to unregulated gastrin release from a non-β cell often well-differentiated neuroendocrine tumour (gastrinoma).
It is most often localized to the duodenum and pancreas. Most gastrinomas occur sporadically, but few are associated with endocrine neoplasia, MEN1 (e.g., pituitary adenomas, parathyroid adenomas, insulinomas).
Most patients present as with recurrent, therapy-resistant peptic ulcer disease and diarrhoea.
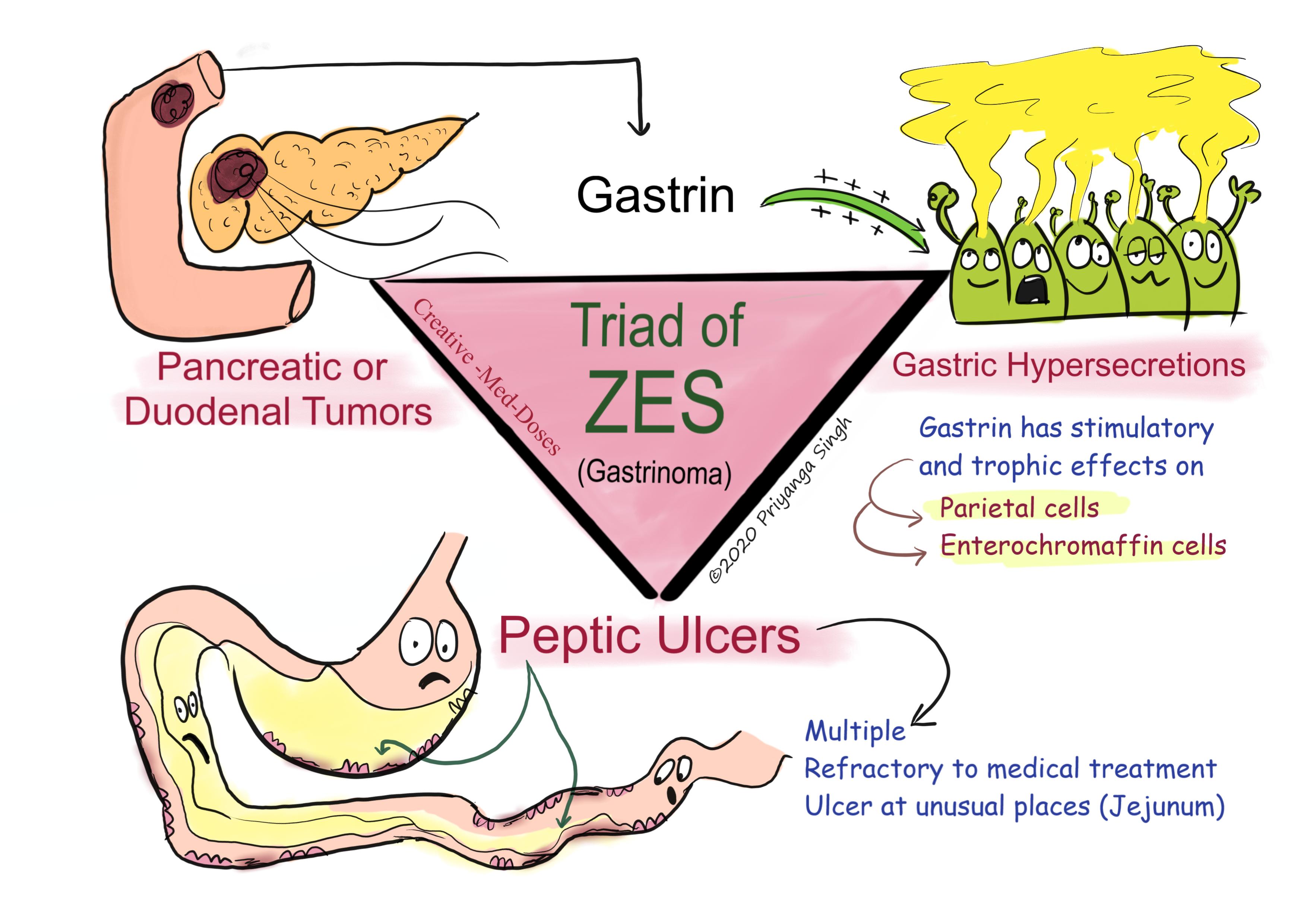
ZES triad
- Pancreatic or duodenal neuroendocrine tumour
- Gastric acid hypersecretion
- Peptic ulcer disease
...
...
Pathophysiology
Hypergastrinemia originating from a neuroendocrine neoplasm is central to all the clinical manifestations in ZES.
Gastrin stimulates acid secretion through gastrin receptors on parietal cells and by inducing histamine release from ECL cells.
Gastrin also has a trophic action (stimulate increase in cell mass) on gastric epithelial cells (parietal cells and enterochromaffin cells).
Longstanding hypergastrinemia leads to markedly increased gastric acid secretion through both parietal cell stimulation and increased parietal cell mass.
The increased gastric acid output leads to peptic ulcer diathesis, erosive esophagitis, and diarrhoea.
Increased acid in intestine leads to inactivation of pancreatic enzymes leading to maldigestion and malabsorption, which causes diarrhoea, steatorrhea, and weight loss.
Tumour location
Gastrinoma Triangle
Over 80%-90% of these tumours are found within the hypothetical gastrinoma triangle (confluence of the cystic and common bile ducts superiorly, junction of the second and third portions of the duodenum inferiorly, and junction of the neck and body of the pancreas medially).
Two most common sites
- Duodenal tumours-constitute the most common nonpancreatic lesion; between 50 and 75% of gastrinomas are found here. Duodenal tumours are smaller, slower growing, and less likely to metastasize than pancreatic lesions.
- Pancreatic tumours- 15-20 % cases of ZES has pancreatic tumours. Pancreatic gastrinomas tend to be solitary, larger and more likely to metastasize.
More than 60% of tumours are considered malignant, with up to 30–50% of patients having multiple lesions or metastatic disease at the time of diagnosis.
Histologically, gastrin-producing cells appear well-differentiated, expressing markers typically found in endocrine neoplasms (chromogranin, neuron-specific enolase).
Clinical Manifestations
Abdominal pain – due to recurrent, refractory and multiple ulcers
Diarrhoea second most common clinical manifestation found in 50% of cases
Etiology of the diarrhoea is multifactorial-
- Marked volume overload to the small bowel (due to increase in acid production)
- Pancreatic enzyme inactivation by acid which leads to maldigestion and malabsorption
- Damage of the intestinal epithelial surface by acid. The epithelial damage can lead to a mild degree of maldigestion and malabsorption of nutrients.
Weight loss – malabsorption and maldigestion leads to weight loss.
Retrosternal pain and Dyspepsia- Symptoms of esophageal origin are present in up to two-thirds of patients with ZES, with a spectrum ranging from mild esophagitis to frank ulceration with stricture and Barrett’s mucosa due to acid reflux.
Ulcers presenting with frank complications, if left untreated
- Bleeding
- obstruction
- perforation
Diagnosis
The presence of refractory, recurrent, multiple and large (> 2-3cm) ulcers in atypical locations (e.g., jejunum) should raise suspicion of gastrinoma.
Measurements of gastrin and acid secretion-
- Hypergastrinemia- fasting serum sample shows↑ Serum gastrin
A gastrin level > 1000 pg/mL (or 10-fold increase in gastrin levels) is conclusive evidence of a gastrinoma. If serum gastrin levels increase (> 100 pg/mL) but are not more than 1000 pg/mL other tests like secretin stimulation test or calcium infusion tests should be performed.
- Low pH- gastric pH <2
Gastrin Provocative tests-
- Secretin stimulation test
(if fasting serum gastrin test is not confirmatory for gastrinoma but degree of suspicion is high)
A two-fold increase in gastrin above the basal level is indicative of a gastrinoma. An increase in gastrin of ≥120 pg within 15 min of secretin injection has a sensitivity and specificity of >90% for ZES.
No increase or only a very slight increase is observed in cases of secondary hypergastrinemia related with
- Calcium infusion study
It is indicated in patients with strong clinical suspicion (recurrent peptic ulcers at unusual locations which are refractory to treatment), which have negative secretin stimulation test.
Imaging
- CT/MRI scan
- somatostatin receptor scintigraphy (octreotide scan)
- endoscopic USG
Treatment
Medical treatment to reduce Acid production –
- High dose of PPI (proton pump inhibitor)
- H2 antagonists (e.g., ranitidine)
- Octreotide for refractory cases which do not respond to PPI and H2 antagonists
Surgical resection of tumour
Chemotherapy for metastatic cases
Revision for today https://creativemeddoses.com/topics-list/hirschsprung-disease-congenital-aganglionic-megacolon/
Buy fun review books here (these are kindle eBook’s you can download kindle on any digital device and login with Amazon accounts to read them). Have fun and please leave review.
Subscribe YouTube channel creative-Med-Doses https://www.youtube.com/channel/UCum2ipWFIH68Xt3houEkyKA