Renal Papillary Necrosis (RPN)
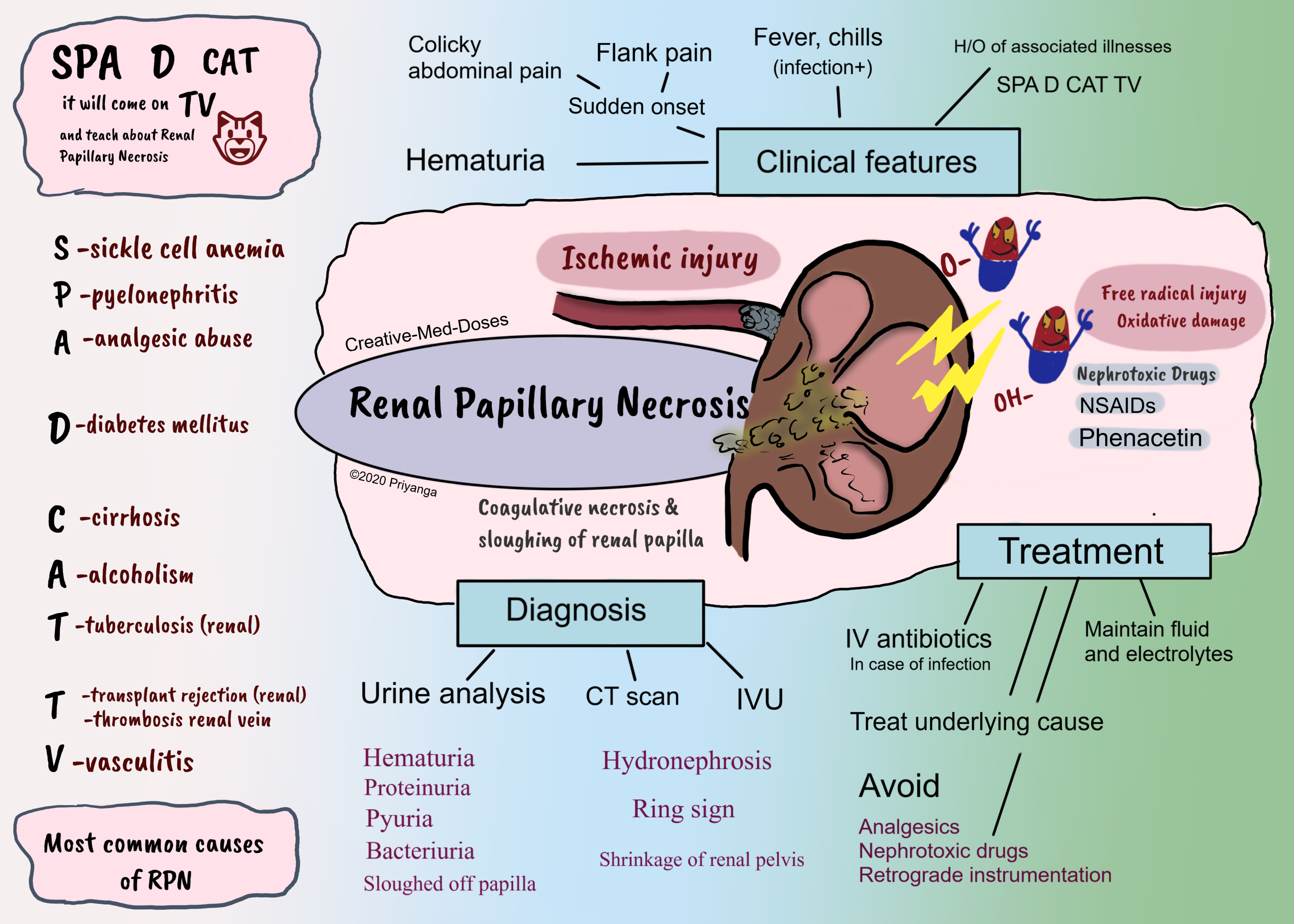
Renal papillary necrosis (RPN) is coagulative necrosis and sloughing off of renal papilla after ischemia or oxidative damage.
The renal papilla is the rounded apex of each medullary pyramid. Each papilla represents the confluence of the collecting ducts from each nephron within that pyramid.
The papillary tip receives only a marginal supply of blood from small-caliber vessels. The already tenuous vascular supply makes renal papilla vulnerable to ischemia and necrosis.
Etiopathogenesis
Reduced blood supply to renal papilla → Ischemia →coagulative necrosis and sloughing of renal papilla → necrosed tissue gets infected or calcified → or it can slough off and obstruct the urinary tract. A large amount of necrosed tissue causes acute urinary tract obstruction and renal failure.
Nephrotoxic drugs can cause renal papillary necrosis by toxic effects and oxidative damage to cells of renal papilla.
The following are the most common causes associated with RPN-
SPA D CAT because it will come on TV and teach Renal Papillary Necrosis
SPA S- sickle cell anemia P- pyelonephritis A- analgesic abuse
D-diabetes Mellitus
C-cirrhosis A-alcoholism T-tuberculosis
T- transplant rejection, thrombosis of renal vein V-vasculitis
Pyelonephritis- the boggy and edematous inflammatory interstitium of pyelonephritis can cause compression of small caliber blood vessels supplying the renal papilla.
Sickle cell hemoglobinopathies
Sickling is common in the renal medulla due to low oxygen tension, low pH, and high osmolality of the renal papilla. Increased blood viscosity due to sickling can lead to infarcts and cause papillary infarcts and coagulative necrosis.
Analgesic abuse (nephropathy)
Diabetes mellitus
Microangiopathy in diabetes mellitus is a precipitating factor for ischemia in small-caliber vessels of renal papilla. The physician should consider sloughed papillae as a cause of ureteral obstruction in the differential diagnoses of flank pain, colic, and hematuria when no calculi are visible and particularly in patients with diabetes.
Clinical features
- Chronic cases are asymptomatic and hydronephrosis is noticed as an incidental finding during a routine investigation
- Sudden onset Flank pain and colicky pain in case of acute obstruction
- Hematuria (microscopic or macroscopic)
- Fever and chills are the sign of infection
In rare cases, there is acute urinary tract obstruction and Acute kidney injury (renal failure)
....
....
Diagnosis
Urine analysis
Hematuria, proteinuria, pyuria, and bacteriuria are the most common findings.
CT scan or Intravenous urography (test of choice for renal papillary necrosis)
findings include:
- Irregular papillae
- Ring shadows
- Contrast material extending into space around a desquamated papilla appears as a” ring shadow” or “lobster claw”.
- Filling defects in the renal pelvis
- Small contrast-containing cavities in the papillary regions
Treatment
Fluid and electrolyte balance
IV antibiotics in case of infection
Treat the underlying cause
Avoid the following-
- Nephrotoxic drugs
- NSAIDs and other analgesics
- Retrograde instrumentation in the urinary tract (as it increases the chances of ascending infection)
Revision for today Barrett’s esophagus - Creative Med Doses
More on Gout Gout: Crystal induced arthropathy - Creative Med Doses