Polymyalgia rheumatica : mournful mornings
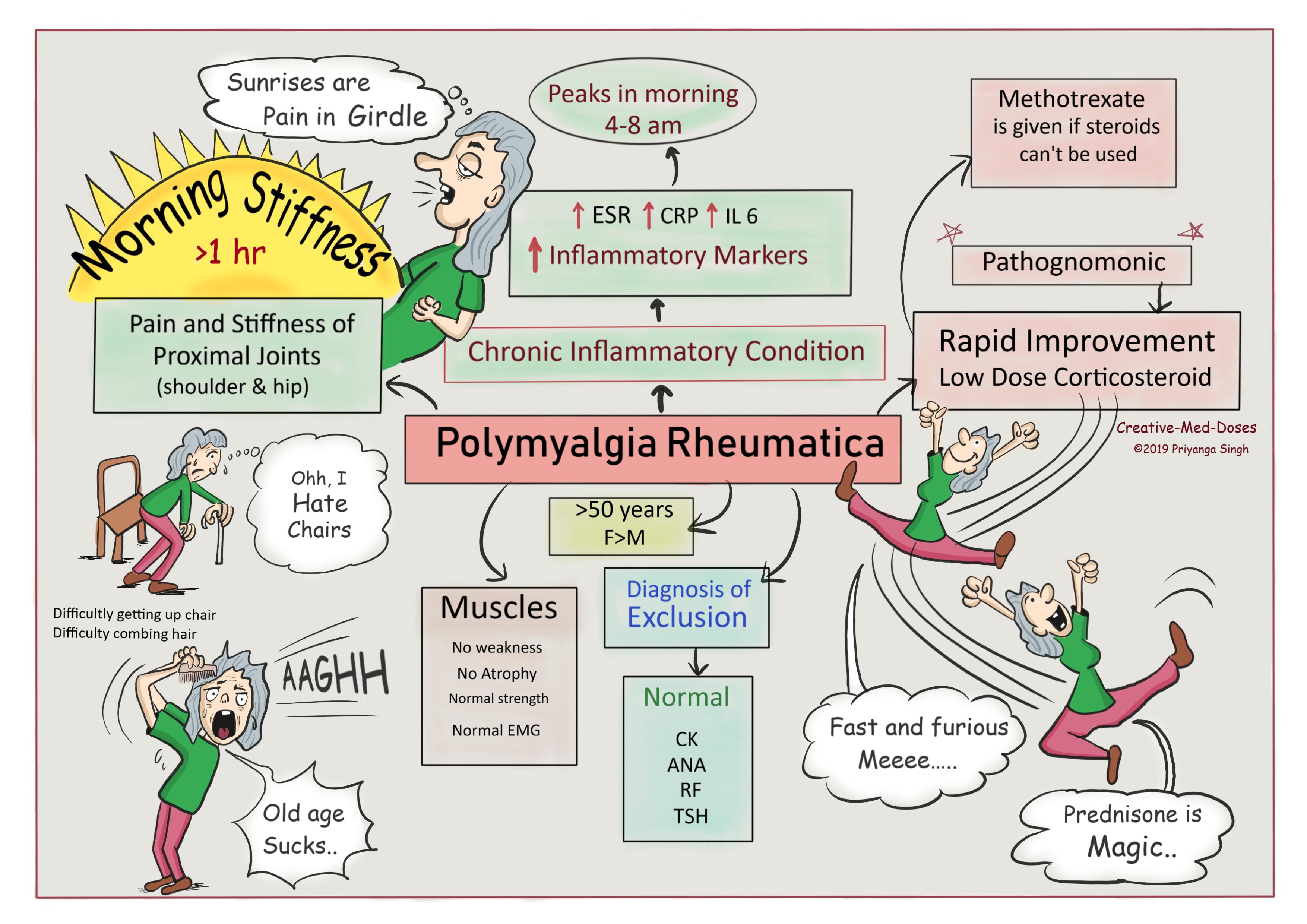
Polymyalgia rheumatica is chronic inflammatory disease of unknown etiology that affects individuals (>50 years). Female to male ratio is 2:1. It is characterized by proximal myalgia of the hip and shoulder girdles with accompanying morning stiffness that lasts for more than 60 minutes.
15-20 % of patients with PMR develop giant cell arteritis.
...
...
Etiology and Pathogenesis
The cause of polymyalgia rheumatica is unknown, but autoimmune, genetic and environmental factors might be responsible.
Most people who are diagnosed with it are over 70 years.
One hypothesis is that in a genetically predisposed patient, an environmental factor, possibly a virus causes monocyte activation. This causes chronic inflammatory state in body raising inflammatory mediators, cytokines (specially IL-6) and ESR. Synovitis, bursitis, and tenosynovitis around the shoulders, hips, knees and metacarpal phalangeal joints are seen in PMR. Systemic macrophage and T-cell activation are characteristic of PMR.
Mornings are painful
The plasma concentrations of IL-6, IL-8, TNF-α, and IL-4 peaks between 4 and 8 am which explains early-morning peak of pain and stiffness in untreated patients.
Muscles are Normal despite excruciating pain
Although PMR causes severe pain and stiffness in the proximal muscle groups, there is no evidence of any abnormality on muscle biopsy. Muscle strength and electromyographic findings are normal and inconclusive.
Clinical Manifestation
- Fatigue
- Low-grade fever
- Weight loss
- Difficulty rising from bed in the morning
- Difficulty getting up from the toilet or out of a chair
- Difficulty completing daily life activities like combing hair
- Morning stiffness for ≥1 hour
- Synovitis of proximal joints
- Joint swelling
- No muscle Atrophy and weakness
- Normal muscle strength
- Rapid response to prednisone (corticosteroid) is pathognomonic.
Diagnosis
It is based on clinical presentation and laboratory studies.
Laboratory studies
- Increased ESR >40mm/hr can exceed 100mm/hr
- Increased CRP (C reactive proteins)
- CBC reveals mild normocytic, normochromic anemia.
- Normal creatine kinase
- Autoantibodies are absent
Treatment
Systemic low-dose corticosteroids- Rapid response to prednisone is pathognomonic.
Methotrexate – reserved for cases where
- Steroids are not effective
- Steroids are contraindicated
Further reading https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2237026/
Revision for today https://creativemeddoses.com/topics-list/behcet-syndrome-ulcers-blindness-and-vasculitis/