Behcet syndrome: Ulcers, Blindness and Vasculitis
Behcet syndrome is a systemic all vessel vasculitis presenting with recurrent oral and genital ulcerations, skin lesions and eye problems are also seen.
...
...
Etiology and pathogenesis
Cause-Unknown/ idiopathic.
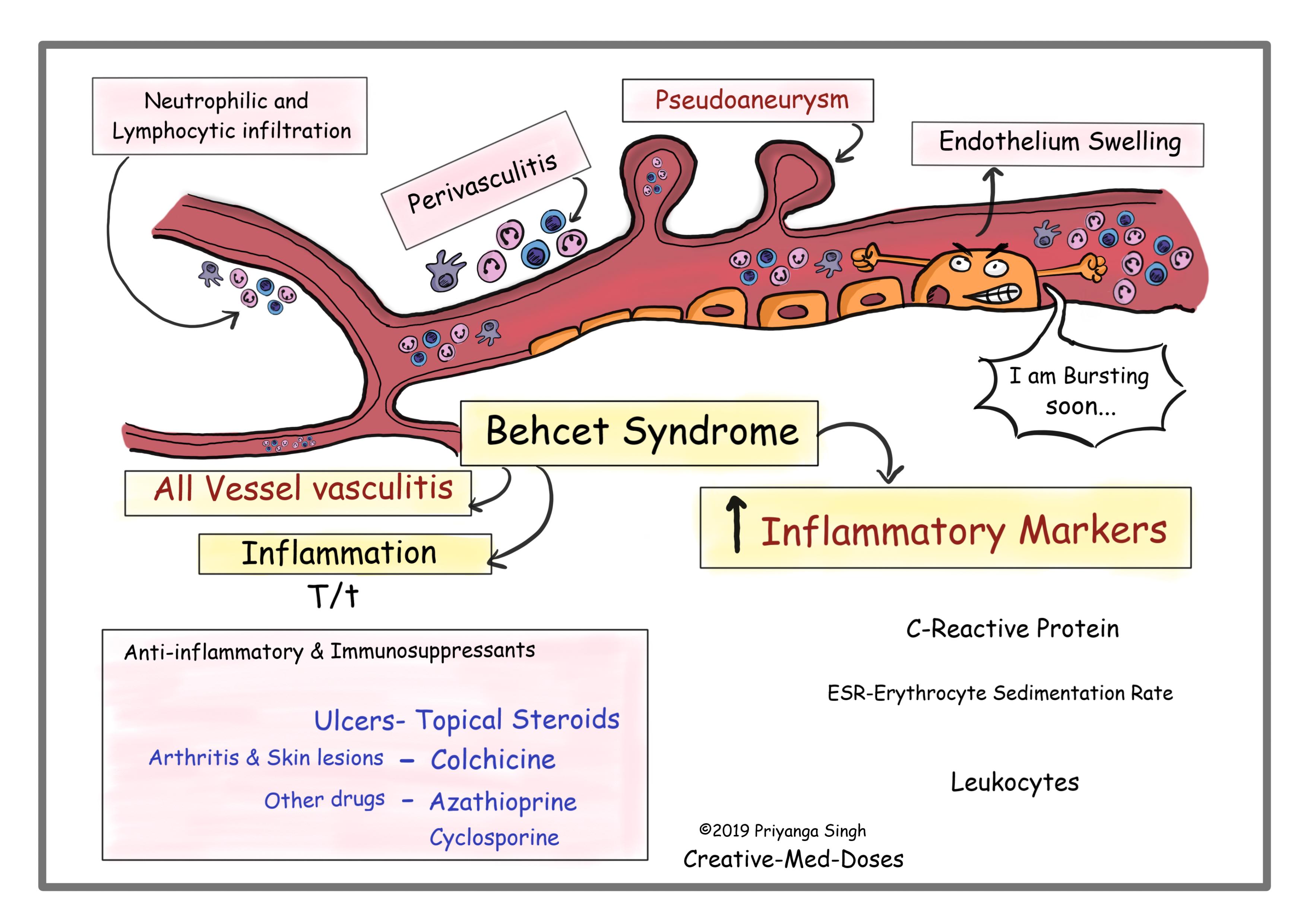
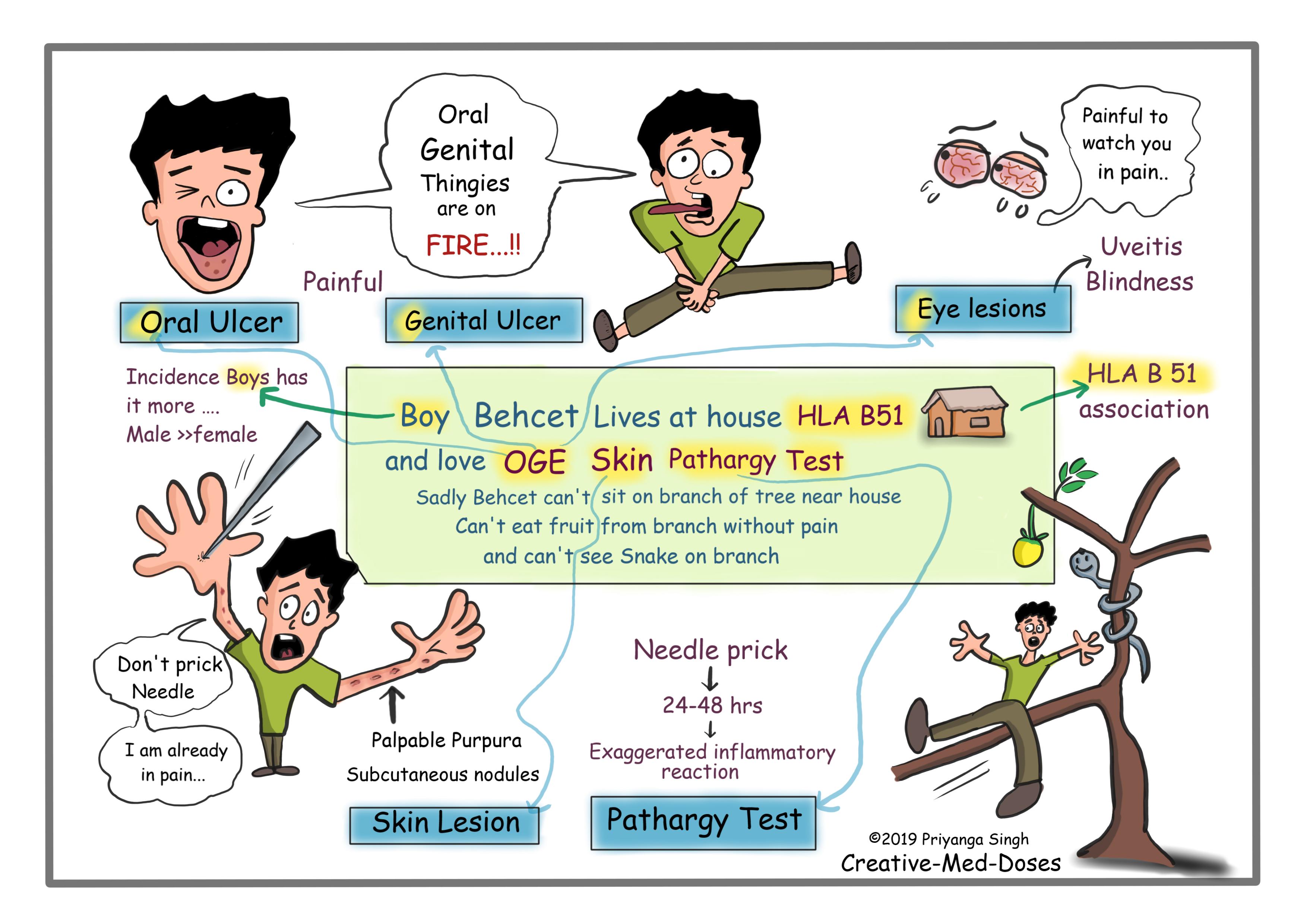
Males are affected more than females and often have severe disease. It is autoinflammatory and autoimmune disorder which has perivasculitis and endothelial swelling in beginning of illness. It can cause diffuse inflammatory disease, which involves all layers of large vessels and leads to formation of pseudoaneurysms and vasculitis of vasa vasorum. Behcet disease patient has increased cytokines, proliferation of T-cells, and hyperactive neutrophils.
Behcet syndrome is associated with HLA-B 51.
Clinical Manifestation and Diagnosis
Diagnostic criteria for Behcet Syndrome
The recurrent oral aphthous ulcerations are a sine qua non for the diagnosis. These ulcers are recurrent painful, with central yellowish necrotic base, they can be located anywhere in the oral cavity. They don’t leave scars after healing.
Plus, any two of following-
- Recurrent genital ulceration- these are painful recurrent ulcers which heals with scarring.
- Ocular lesions- Uveitis and iritis are commonly seen. Bilateral pan uveitis is the most dangerous complication, because it can rapidly progress to blindness.
- Skin lesions – Folliculitis, erythema nodosum, acne-like rashes, palpable purpura and subcutaneous nodules are seen in 80% of the cases.
- Positive Pathergy test- Pathergy is an exaggerated skin injury following minor trauma such as bump, bruise, needle stick injury. Multiple pricks are made into the forearm, using a sterile needle. The pricked area is observed after 24-48 hours. The development of an inflammatory papule or pustule within 24-48 hours constitutes a positive result. Positive Pathergy test result is indicator of an overactive immune response to minor injuries.
Diagnosis
Most cases are clinically diagnosed based on above diagnostic criteria.
Lab results show increased inflammatory markers such as erythrocyte sedimentation rate, C-reactive protein and leukocytes.
Biopsy from ulcers shows leukocytoclastic vasculitis or lymphocytic vasculitis and perivasculitis with neutrophil infiltration and endothelial swelling.
Treatment
Topical corticosteroids for ulcers
Colchicine
Other systemic immunosuppression- cyclosporine, infliximab, cyclophosphamide, or azathioprine can be used in more severe cases.
Case scenario
...

...
A 42-year-old man presents to clinician with recurrent painful oral and genital ulcers. He also reports blurring of vision and joint stiffness. On physical examination, five aphthous ulcers are seen with yellow debris and erythematous border. Genital exam reveals scarring and multiple erythematous ulcers. His STD screening is negative, and he isn’t HIV positive. He also reports joint stiffness and pain. His blood test shows increased ESR and C-reactive proteins. Which is most appropriate treatment for his ulcers?
- Topical steroids
- Topical analgesics
- Fluconazole
- Probiotics
Further reading https://www.onlinelibrary.wiley.com/doi/full/10.1002/ccr3.79
Revision for day https://creativemeddoses.com/topics-list/alport-syndrome-type-iv-collagen-defect/