Alport Syndrome – Type IV collagen defect
Alport syndrome is a rare genetic disorder characterized by progressive hereditary nephritis with hematuria secondary to basement membrane disease of the glomeruli. It is a type of hereditary nephritis with high-frequency sensorineural hearing loss (SNHL) and pathognomonic ocular lesions (Lenticonus).
...
...
Pathogenesis
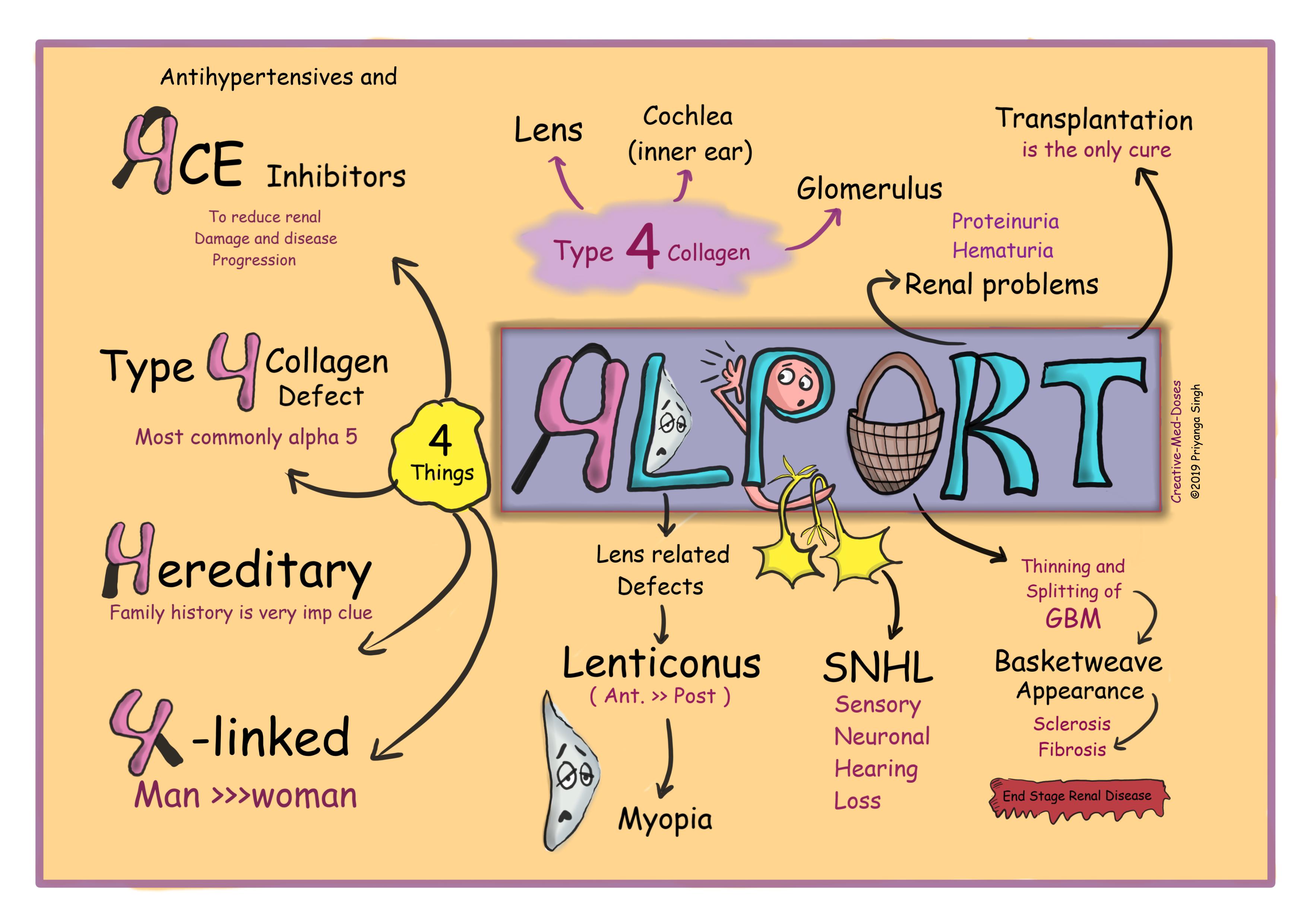
The most common mode of inheritance is X-linked, and men are more severely affected (obviously like most X-linked diseases).
Collagen type IV mutation that results in an abnormal basement membrane. Type IV collagen is crucial for normal function of the lens, cochlea, and glomerulus. It is made up of heterotrimers of α3, α4, and α5 chains. Mutation of any one of the α chains results in defective heterotrimer composition and manifest as Alport syndrome.
collagen α5 chain is the most commonly affected one in Alport Syndrome. (60-70% cases).
Clinical manifestation
Renal involvement
Renal biopsy appear unremarkable until late in the course. With progression of illness there will be glomerulosclerosis, vascular sclerosis, tubular atrophy, and interstitial fibrosis. These changes lead to end stage renal disease and renal failure.
Electron microscopy reveals GBM (glomerular basement membrane thinning and splitting with irregular foci of thickening yielding a “basket weave” appearance.
Microscopic or frank hematuria persistent from childhood constitutes the clinical clue for its early recognition. Patient presents with hematuria and proteinuria.
Ocular involvement
Anterior lenticonus is a hallmark for ocular manifestation of AS. However, posterior lenticonus is also seen in some cases. Lens capsule has three-dimensional molecular meshwork, primarily of type IV collagen and other extracellular matrix constituents. Mutation in the gene that codes for type IV collagen results in capsule fragility, leading to conical protrusion of the capsule at its weakest point which is giving rise to lenticonus. Anterior lenticonus is more commonly seen than posterior, which leads to progressive lenticular myopia developing by the second decade as seen in our patient.
Dot and fleck retinopathy is also seen in few cases.
Hearing defect
Progressive sensorineural hearing loss beginning with high frequencies.
Diagnosis
Clinical presentation, family history and Renal biopsy are center of diagnosis. Confirmation of disease can be achieved by genetic analysis.
Treatment
No cure is available except renal transplantation for end stage renal disease and intraocular lens implantation for lenticonus.
Supportive treatment –
antihypertensive and
ACE inhibitors for slowing disease progression.
Case scenario
A 16-year-old boy is brought to physician office by grandfather with chief complaints of hematuria, problems with vision, and deafness. Family history is significant for deafness and his father died of hypertension related cerebral hemorrhage. His temperature is normal, blood pressure is 160/100 mmHg, pulse is 75/min, and respirations are 17/min. Physical examination reveals anterior lenticonus and sensorineural hearing loss. Urinalysis demonstrates dysmorphic red blood cells and red blood cell casts. What is most likely diagnosis. What is expected renal biopsy finding in this case??
Further reading https://ghr.nlm.nih.gov/condition/alport-syndrome
Revision for today https://creativemeddoses.com/topics-list/fragile-x-syndrome-x-linked-mr/