Irritable bowel syndrome: Stress and diarrhea
Irritable bowel syndrome (IBS) is a functional gastrointestinal disorder characterized by recurrent abdominal pain and altered bowel habit in the absence of significant organic pathology.
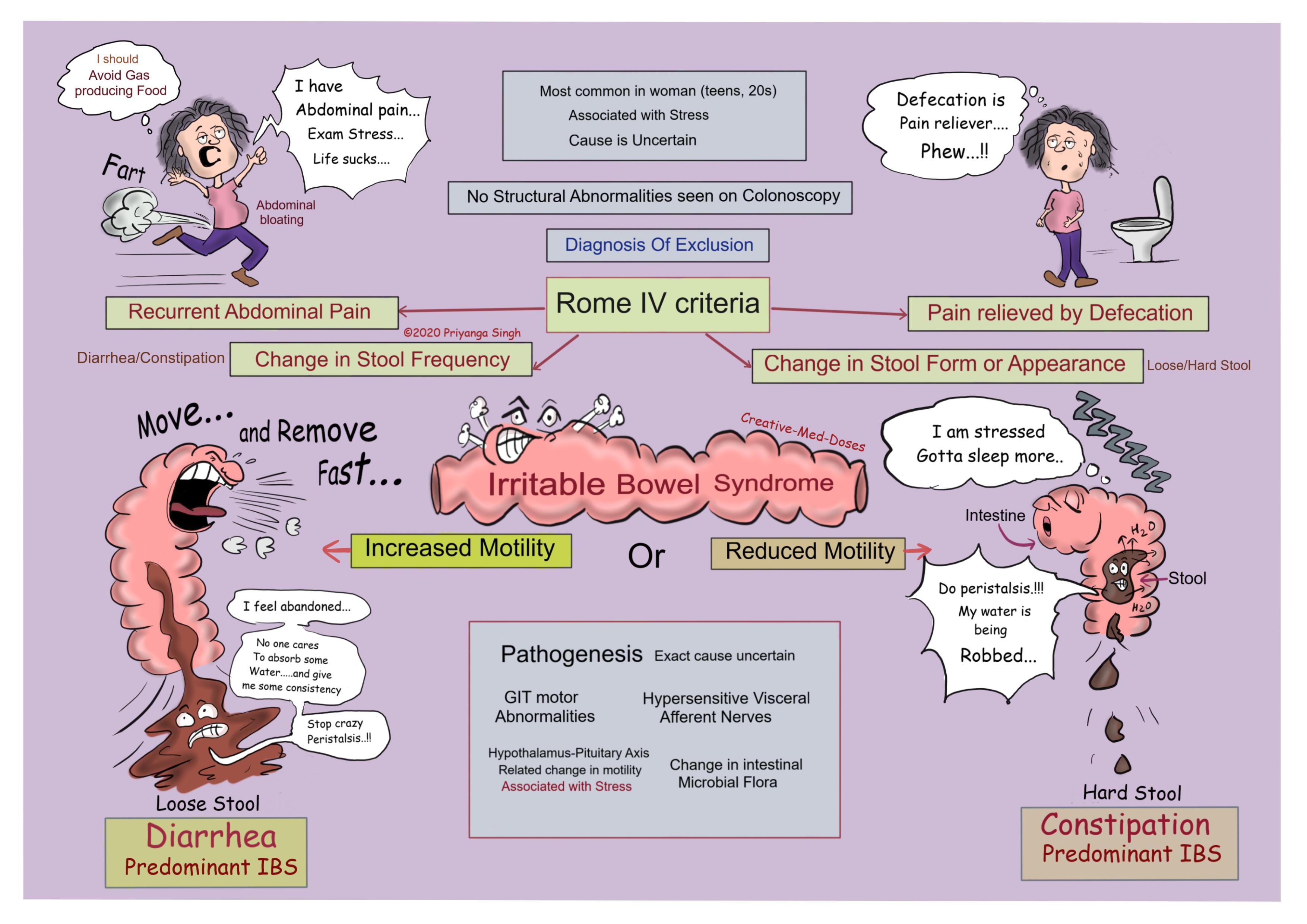
Pathogenesis
Irritable bowel syndrome has no significant structural abnormality and pathogenic mechanism causing disease is uncertain.
Following are few hypotheses associated with IBS-
- Gastrointestinal tract motor abnormalities (e.g., abnormal transit time). Small bowel dysmotility manifests in delayed meal transit in patients prone to constipation and in accelerated meal transit in patients prone to diarrhea.
- Hypersensitization of visceral afferent nerves in the gut, which can affect peristalsis and thus bowel movements.
- The hypothalamic-pituitary axis may be intimately involved in the pathogenesis of IBS. Motility disturbances correspond to an increase in hypothalamic corticotropin-releasing factor (CRF) production in response to stress. Comorbid psychiatric disease (e.g., major depression or anxiety) also affects this axis and thus leads to abnormal intestinal motility.
- Alterations in the intestinal microbiota
Clinical features
- Recurrent Abdominal Pain- Meals may precipitate pain, and defecation commonly improves pain. It can be stimulated with stress or meals.
- Altered bowel habits- Constipation results in complaints of hard stools of narrow caliber, painful or infrequent defecation, and intractability to laxatives. Diarrhea usually is described as small volumes of loose stool, with evacuation preceded by urgency or frequent defecation.
- Abdominal distention- there is bloating and increased gas production in IBS, avoiding gas producing foods can give relief in bloating and distention.
Diagnosis
The Rome IV criteria for the diagnosis of irritable bowel syndrome require that patients have had recurrent abdominal pain on average at least 1 day per week during the previous 3 months that is associated with two or more of the following--
- Related to defecation (pain relieved by defecation)
- Associated with a change in stool frequency
- Associated with a change in stool form or appearance
...
...
Treatment
- Lifestyle Modifications – reduced consumption of gas producing food, Fiber supplementation may improve symptoms of constipation and diarrhea.
- Psychiatric Treatment
- Laxatives--Lubiprostone is indicated in patients with moderate to severe IBS with constipation.
- Antidiarrheal agents --loperamide is indicated in patients with moderate to severe IBS with diarrhea.
- Antispasmodics--dicyclomine is used on a as needed basis for IBS-related abdominal pain.
Case Scenario
A 25-year-old woman presents to the clinic with chief complaints of intermittent abdominal pain and occasional episodes of diarrhea for 3 months. She reports that the pain would improve partially after she defecates or when she is relaxed. It is much worse now as she is feeling depressed and stressed out because of recent breakup and failure in exam. Her gastrointestinal workup including fecal leukocytes, stool culture, fecal RBCs, and colonoscopy reveals no abnormalities.
Which drug is Most likely to relieve symptoms?
- Bismuth subsalicylate
- Polyethylene glycol
- Loperamide
- Lubiprostone
Further reading https://www.physio-pedia.com/Irritable_Bowel_Syndrome
Revision for today https://creativemeddoses.com/topics-list/hereditary-spherocytosis-intrinsic-hemolysis/