Hereditary Spherocytosis: Intrinsic Hemolysis
Hereditary spherocytosis (HS) is the most common inherited red cell membrane disorder causing chronic hemolytic anemia. This defect lead to the formation of spherocytes, which are nondeformable cells.
Pathogenesis
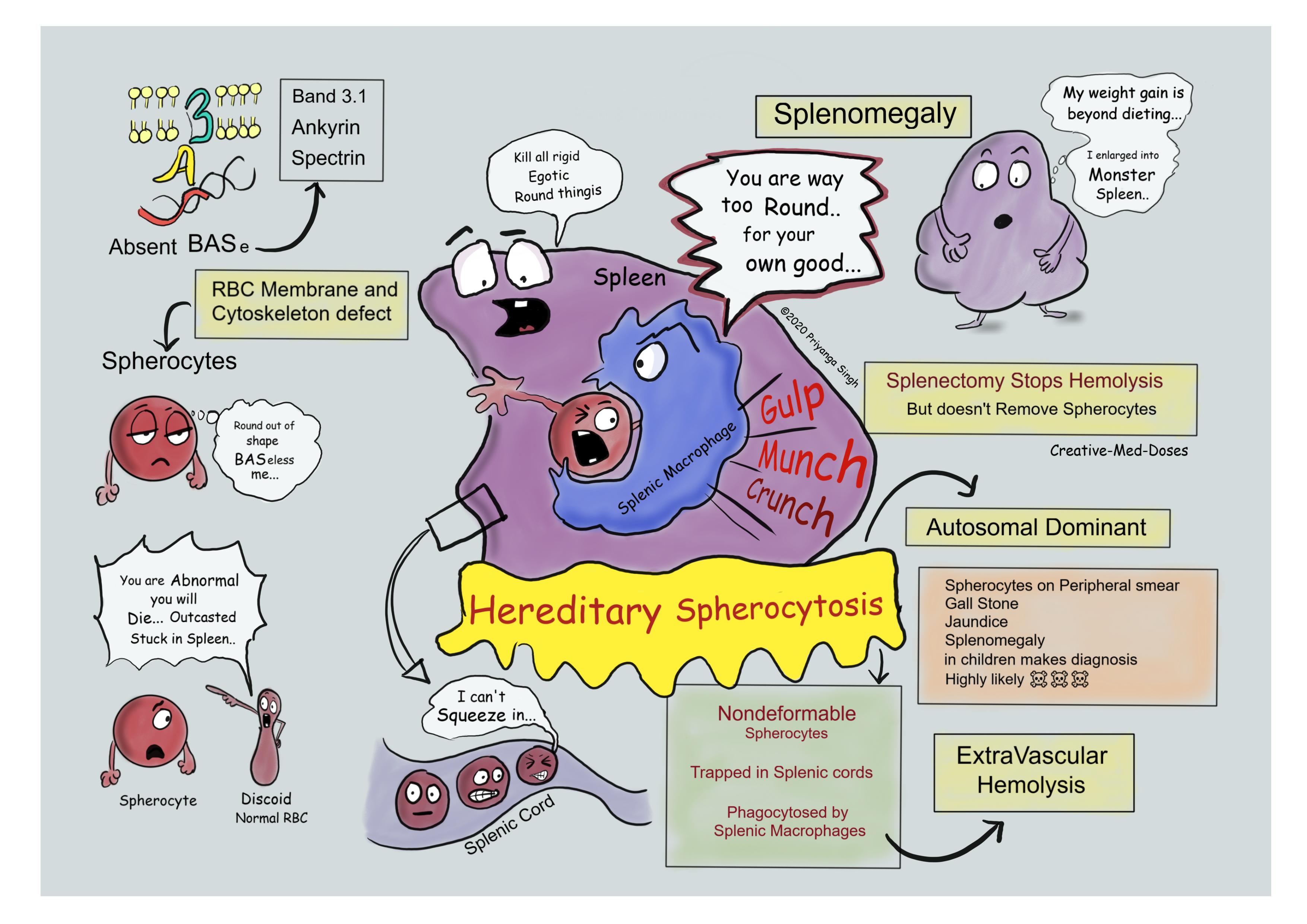
It is commonly inherited in autosomal dominant pattern. It caused by a deficiency in red blood cell membrane proteins spectrin, ankyrin, or Band 3.1. These are major proteins that act as cytoskeleton of the red blood cell and as a result of defective membrane, red blood cells become spherically shaped.
The nondeformable spherocytes become trapped in the spleen as they course through the sinuses, and these trapped spherical red cells are engulfed by macrophages causing hemolysis.
Red cells must undergo extreme degrees of deformation to pass through the splenic cords. The discoid shape of normal red cells allows them to deform themselves and squeeze out from splenic cords, but spherocytes have limited deformability and are sequestered in the splenic cords and are eventually destroyed by the splenic macrophages. Splenomegaly is very characteristic feature of HS.
The excessive red cell destruction and hemolytic anemia lead to a compensatory hyperplasia of red cell progenitors in the marrow and an increase in red cell production marked by reticulocytosis.
The splenic enlargement occurs due to marked congestion of splenic cords and increased number of macrophages.
Clinical Features
- Anemia
- Splenomegaly- mild to moderate splenomegaly is very characteristic and common presenting feature.
- Jaundice- increased hemolysis causes hyperbilirubinemia and jaundice.
- Cholelithiasis- increased hemolysis causes increased indirect bilirubin in the bile, which leads to formation of pigmented calcium bilirubinate stones.
- Aplastic crises- It is triggered by parvovirus B19 infection in most cases. This virus infects erythroblasts and causes apoptosis during viral replication. The infection by parvovirus B19 leaves bone marrow virtually devoid of red cell progenitors(erythroblasts). Because of the shortened life span of red cells in hereditary spherocytosis, this lack of red cell production results in rapid worsening of the anemia and presents as Aplastic crises. Blood transfusions may be needed to support patients.
Diagnosis
- Peripheral blood smear- normocytic anemia with spherocytes which lack central pallor, smaller and rounder than normal Red Blood Cells.
- Reticulocyte count- increased turnover of RBCs in response to hemolysis causes significant reticulocytosis and increased Reticulocyte count.
- Indirect bilirubin- is increased due to excessive extravascular hemolysis.
- Osmotic Fragility Test- Because of their spherical shape, red cells in hereditary spherocytosis show increased osmotic fragility when placed in hypotonic salt solutions.
...
...
Treatment
- There is no cure, but following treatment helps in disease severity.
- Splenectomy- Severe disease requires hematological supervision and may benefit from splenectomy, which should be performed after the age of 6 years. Risk of infections post splenectomy should be weighed against disease severity, especially in children younger than 6 years.
- Folic acid and B12 supplementation- increased cell turnover in hemolytic anemia might cause deficiency of Folic acid and B12 so supplements prevents deficiency of these vitamins.
Case Scenario
A 12-year-old boy presents to pediatrician with Right upper quadrant pain and tenderness. Physical Exam shows mild splenomegaly and jaundice. His labs show a mild normocytic anemia with an elevated reticulocyte count. Peripheral blood smear shows that many of his RBCs have no area of central pallor and are smaller than normal RBCs. Ultrasound abdomen reveals few gall stones and splenomegaly. Which is most likely diagnosis? Explain formation of gall stones in this case?
Further reading https://bestpractice.bmj.com/topics/en-gb/1143
Revision for today https://creativemeddoses.com/topics-list/inflammatory-bowel-disease-ibd-pathogenesis/