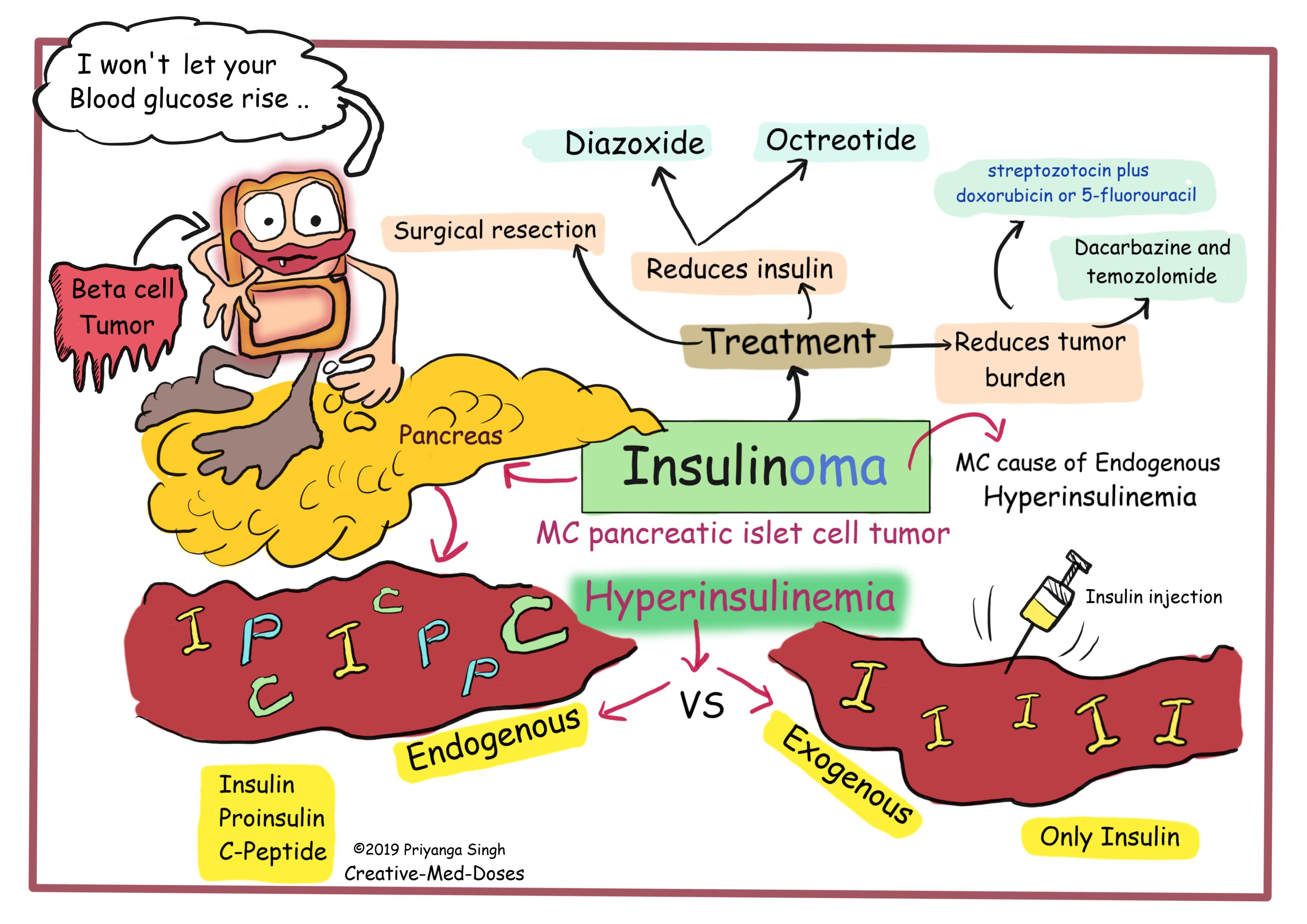
Insulinoma – Beta cell tumor
An insulinoma is NET (neuroendocrine tumors) of the pancreas, derived from beta cells that ectopically secrete insulin, which results in hypoglycemia. Insulinoma is a rare pancreatic islet cell tumor, the most common cause of hypoglycemia related to endogenous hyperinsulinism. Most insulinomas are solitary and benign. The average age of occurrence is 40–50 years old.
Clinical manifestation
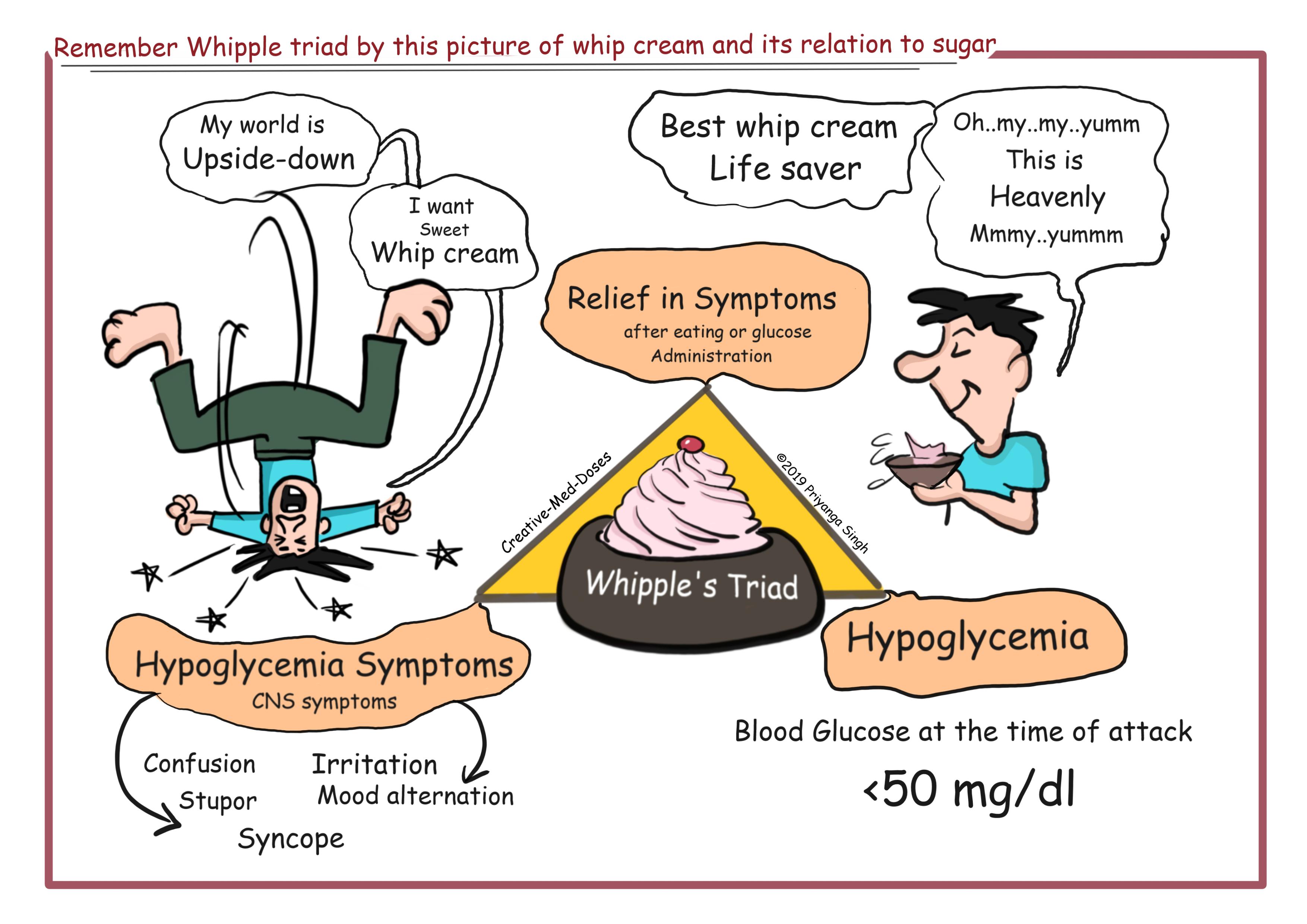
These attacks manifest as confusion, stupor, and loss of consciousness. They are precipitated by fasting or exercise and are promptly relieved by feeding or parenteral administration of glucose. The most common clinical symptoms are due to the effect of the hypoglycemia on the CNS (neuroglycemic symptoms) and include confusion, headache, disorientation, visual difficulties, irrational behavior, and even coma. Also, most patients have symptoms due to excess catecholamine release secondary to the hypoglycemia, including sweating, tremor, and palpitations. Characteristically, these attacks are associated with fasting.
Insulinomas should be suspected in all patients with hypoglycemia, especially when there is a history suggesting that attacks are provoked by fasting, or with a family history of MEN 1.
Insulin is synthesized as proinsulin, which consists of a 21-amino-acid α chain and a 30-amino-acid β chain connected by a 33-amino-acid connecting peptide (C peptide). In insulinomas, in addition to elevated plasma insulin levels, elevated plasma proinsulin levels are found, and C-peptide levels are elevated.
Diagnosis
The diagnosis of insulinoma requires the demonstration of an elevated plasma insulin level at the time of hypoglycemia. The most reliable test to diagnose insulinoma is a fast up to 72 h with serum glucose, C-peptide, proinsulin, and insulin measurements every 4–8 h. Some 70–80% of patients will develop hypoglycemia during the first 24 h, and 98% by 48 h. A commonly used set of criteria to make the diagnosis include: low blood glucose levels (≤2.2 mmol/L (≤40 mg/dL); concomitant insulin levels ≥6 U/L (≥ 36 pmol/L; ≥3 U/L by ICMA); C-peptide levels ≥200 pmol/L; proinsulin levels ≥5 pmol/L; β-hydroxybutyrate levels ≤2.7 mmol/L; and absence of sulfonylurea (metabolites) in the plasma and/or urine.
Surreptitious use of insulin or hypoglycemic agents may be difficult to distinguish from insulinomas. The combination of proinsulin levels (normal in exogenous insulin/hypoglycemic agent users), C-peptide levels (low in exogenous insulin users), antibodies to insulin (positive in exogenous insulin users), and measurement of sulfonylurea levels in serum or plasma will allow the correct diagnosis to be made. In these patients, the assessment of proinsulin and C-peptide levels at the time of hypoglycemia is particularly helpful for establishing the correct diagnosis. An elevated proinsulin level when the fasting glucose level is <45 mg/dL is sensitive and specific.
Treatment
Localized tumor needs surgery-Laparoscopic Enucleation, or partial pancreatic resection if the tumor is localized.
Medical therapy is indicated in patients with malignant insulinomas and in those who will not or cannot undergo surgery.
To prevent hypoglycemia
- Small frequent meals
- Diazoxide- reduces insulin secretion.
- Octreotide- reduces insulin secretion.
To reduce tumor burden
- Combination therapy with streptozotocin plus doxorubicin or 5-fluorouracil
- Dacarbazine and temozolomide based regimens
...
...
Stay tuned for more funmed updates 😍.
Further reading https://www.oatext.com/pancreatic-insulinoma-case-report-and-review-of-the-literature.php
Revision for today https://creativemeddoses.com/topics-list/whipples-disease-diarrhea-with-dementia/