Whipple’s disease-Diarrhea with Dementia
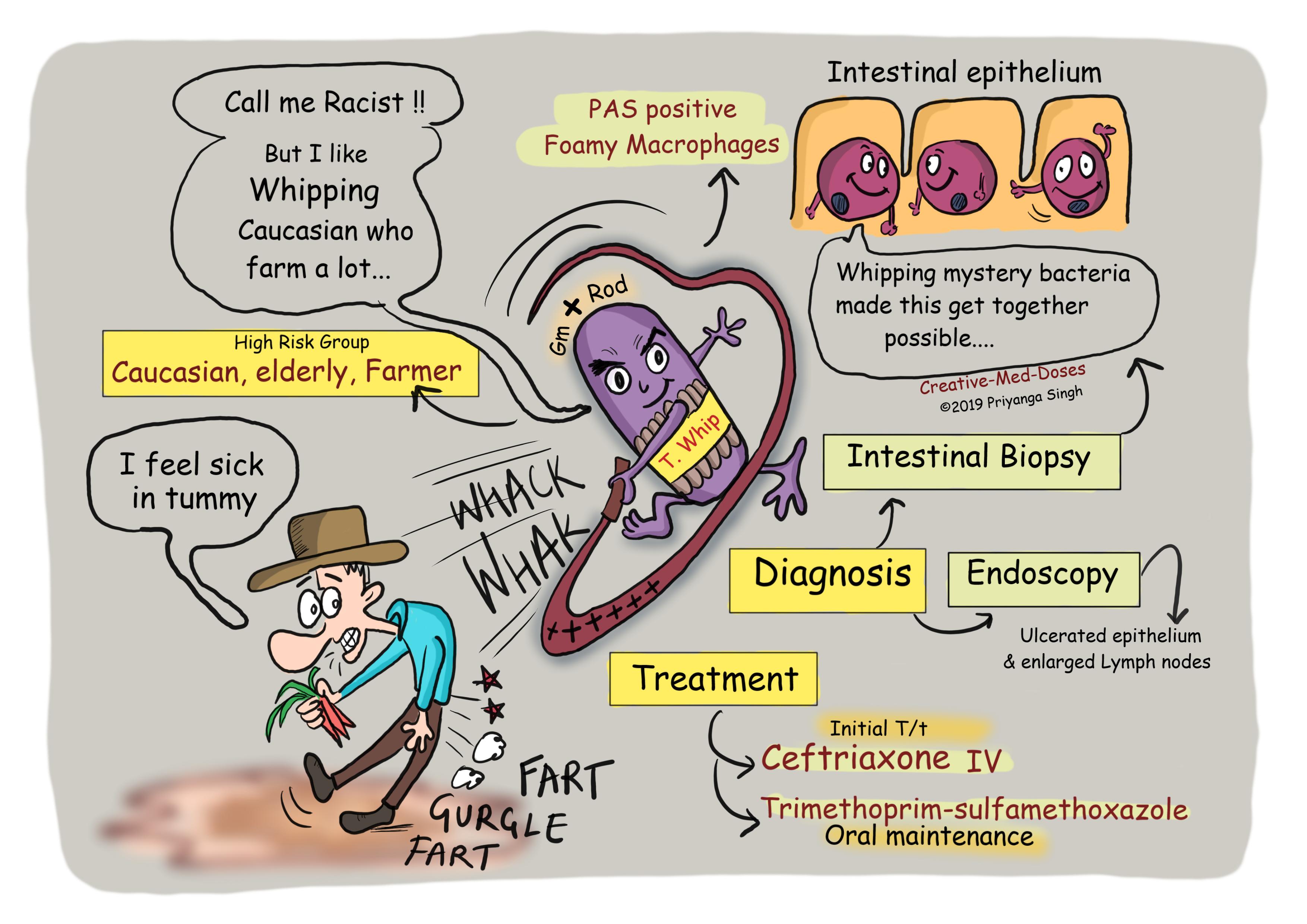
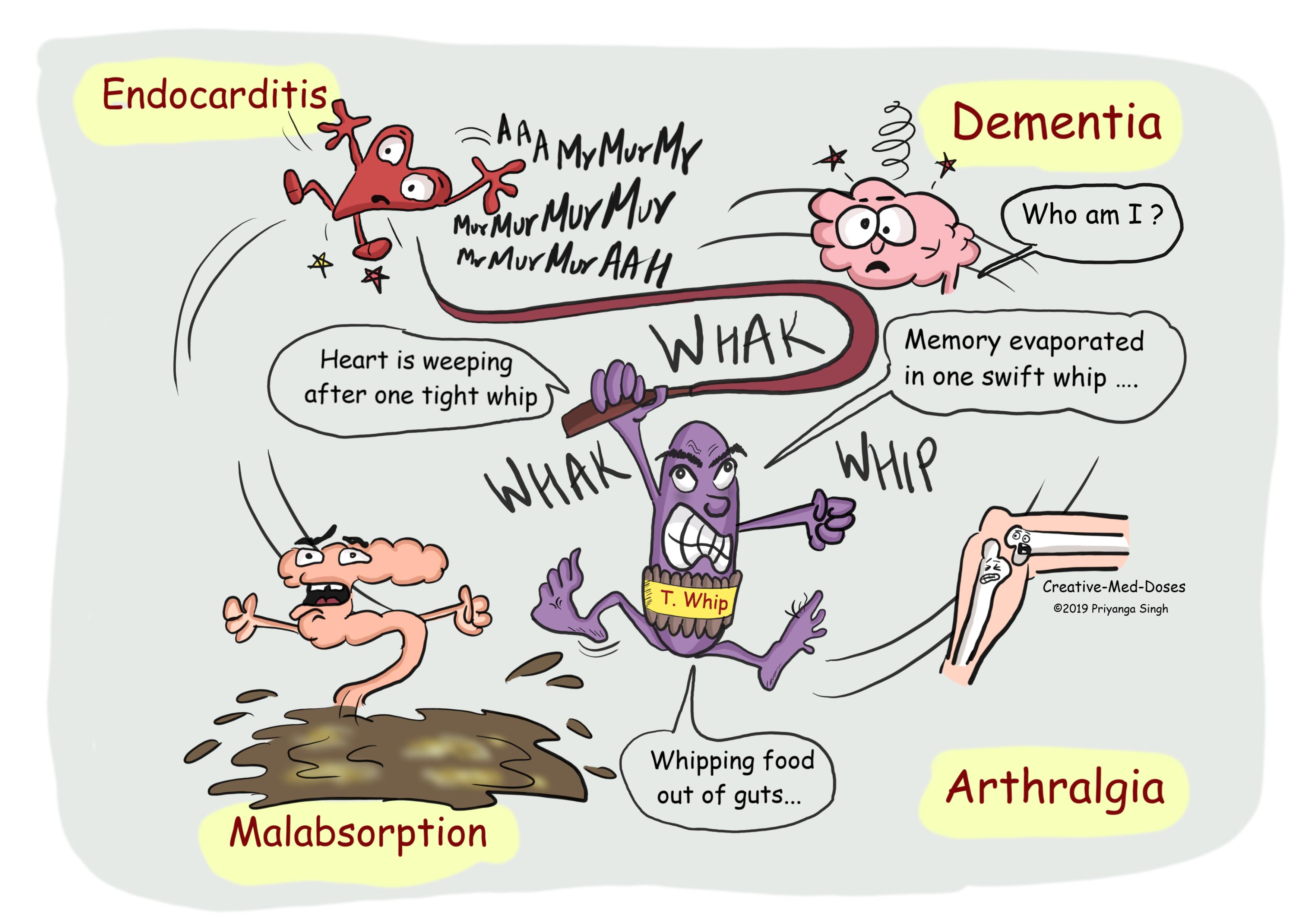
Whipple’s disease is a chronic infection caused by Tropheryma whipplei. T. whipplei is a weakly staining gram-positive bacillus. It has predilection for causing disease in middle-aged Caucasian men who are farmers. Whipple's disease mainly causes malabsorption but may affect other parts of the body including the heart, brain, joints, skin, lungs and the eyes.
...
...
...
Pathogenesis
The defective T-lymphocyte (Helper T cells/TH1 cells) function may be an important predisposing factor for the disease. This dysfunction along with macrophage phagocytosis defects leads to accumulation of bacteria in organs, which leads to inflammation and injury to the tissue involved.
T. whipplei has a tropism for myeloid cells. It invades myeloid cells and stays there to avoid being killed. Infiltration of infected tissue by large numbers of foamy macrophages containing periodic acid–Schiff (PAS)–staining inclusions (representing ingested bacteria) is a characteristic and most common finding. As the disease progress, there will be villus atrophy, lymphangiectasia, crypt hyperplasia, and apoptosis of surface epithelial cells of small intestine. The epithelium destruction of small intestine leads to diarrhea due to decreased absorption and increased leak flux of water and solutes. Malabsorption of nutrients is responsible for weight loss and fat-soluble vitamin deficiency.
Clinical manifestation
Asymptomatic Colonization-The prevalence of fecal carriage is high in individuals with exposure to wastewater or sewage, and they are carriers for the disease without exhibiting any symptoms.
Acute infection- Acute gastroenteritis is common in children and manifest as fever and diarrhea.
Chronic infection-
Classic whipple’s disease- involves joints (arthralgia), CNS (dementia and seizures), intestine (malabsorption, diarrhea, steatorrhea, weight loss).
Neurological- The most common are cognitive changes progressing to dementia, personality and mood alterations, hypothalamic involvement, and supranuclear ophthalmoplegia. Supranuclear gaze palsy, oculomasticatory and oculofacial myorhythmia (highly suggestive of Whipple’s), and nystagmus is also seen.
Cardiac- Endocarditis, valve defects.
Pulmonary-interstitial disease, nodules, parenchymal infiltrate, and pleural effusion may be seen.
Diagnosis
Endoscopic small bowel biopsy – It is the most accurate test which reveals PAS-positive macrophages in the lamina propria containing non-acid-fast gram-positive bacilli.
Endoscopy reveals pale yellow shaggy mucosa with erythematous eroded patches(enanthema) in patients with classic intestinal Whipple's disease.
Immunohistochemical staining for antibodies against T. whipplei can be done.
PCR on blood, vitreous fluid, synovial fluid or cerebrospinal fluid can be confirmatory.
Treatment
Long term antibiotic course is needed in most cases. Initially intravenous treatment with penicillin/ceftriaxone is given and oral trimethoprim-sulfamethoxazole is used as maintenance therapy.
Further Reading https://newbp.bmj.com/topics/en-us/467
Revision for today https://creativemeddoses.com/topics-list/sjogren-syndrome-dry-eyes-and-dry-mouth/