Gitelman syndrome: NCCT defect
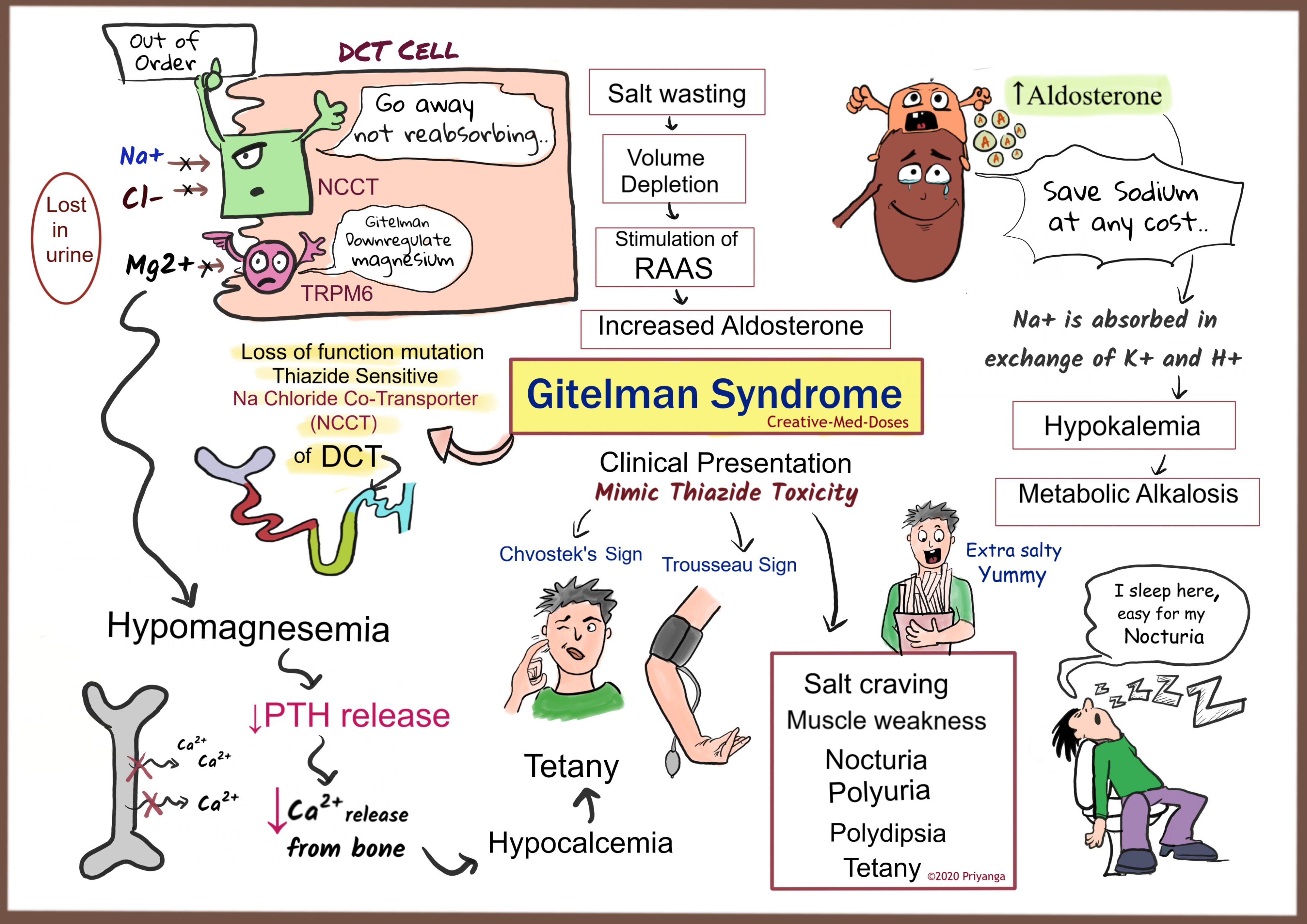
Gitelman syndrome (GS) is also known as familial hypokalemic hypomagnesemia with hypocalciuria. It is an autosomal recessive hereditary salt-losing tubulopathy. It is characterized by hypokalemic metabolic alkalosis, hypomagnesemia, and hypocalciuria. The disease is caused by mutations in the SLC12A3 gene encoding the thiazide-sensitive sodium chloride cotransporter (loss of function mutations in NCCT).
Pathogenesis
Loss of function Mutation causing NCCT failure, Salt-wasting, and rescue mechanism causing hypokalemia and metabolic alkalosis
In Gitelman syndrome less sodium is reabsorbed in the DCT due to the defective NCCT, the increased sodium delivery to the collecting duct causes a degree of distal sodium rescue, resulting in increased potassium and hydrogen excretion, and therefore the characteristic biochemical picture of hypokalaemia and metabolic alkalosis.
Hypomagnesemia, PTH, and Hypocalciuria
Gitelman syndrome also has down‐regulation of the apically located transient receptor potential channel 6 (TRPM6), a magnesium‐permeable channel predominantly expressed in the DCT. It causes hypomagnesemia.
Reduced levels of magnesium in the blood inhibit the release of parathyroid hormone, which can result in hypoparathyroidism and hypocalcemia.
Hypocalcemia and tetany
Low ionized calcium levels in the extracellular fluid increase the permeability of neuronal membranes to sodium ion, causing a progressive depolarization, which increases the possibility of action potentials causing tetany.
Tetany is characterized by contraction of distal muscles of the hands (carpal spasm with the extension of interphalangeal joints and adduction and flexion of the metacarpophalangeal joints) and feet (pedal spasm) and is associated with tingling around the mouth and distally in the limbs.
Clinical presentation
The clinical manifestations of GS are highly variable and differ in age at presentation, the severity of symptoms, and biochemical abnormalities.
Patients are usually diagnosed in adulthood during a routine investigation.
The most common symptoms were salt craving, with musculoskeletal symptoms such as cramps, muscle weakness, and aches, and constitutional symptoms such as fatigue, generalized weakness and dizziness, and nocturia and polydipsia. Tetanic episodes in severe cases of hypocalcemia and hypomagnesemia.
...
...
Diagnosis
Blood tests shows -
- hypokalemia
- hypomagnesemia
- metabolic alkalosis
Urine studies
- Increased loss of potassium, magnesium, and sodium in the urine
- ↓ Ca2+
Genetic testing is confirmatory
Treatment
Electrolyte replacement
- Maintaining the Electrolyte balance is the cornerstone of the treatment
- Rapid clinical and biochemical improvement can be achieved by replacement therapy with potassium and magnesium.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
- indomethacin
- celecoxib
Potassium-sparing diuretics
they are given to treat hypokalemia and metabolic alkalosis
- amiloride
- eplerenone
Revision for today https://creativemeddoses.com/topics-list/iga-nephropathy-berger-disease/
Follow us on Facebook https://www.facebook.com/creativemeddoses
Buy fun review books here (these are kindle eBooks you can download kindle on any digital device and log in with Amazon accounts to read them). Have fun and please leave a review.