Contrast-Induced Nephropathy
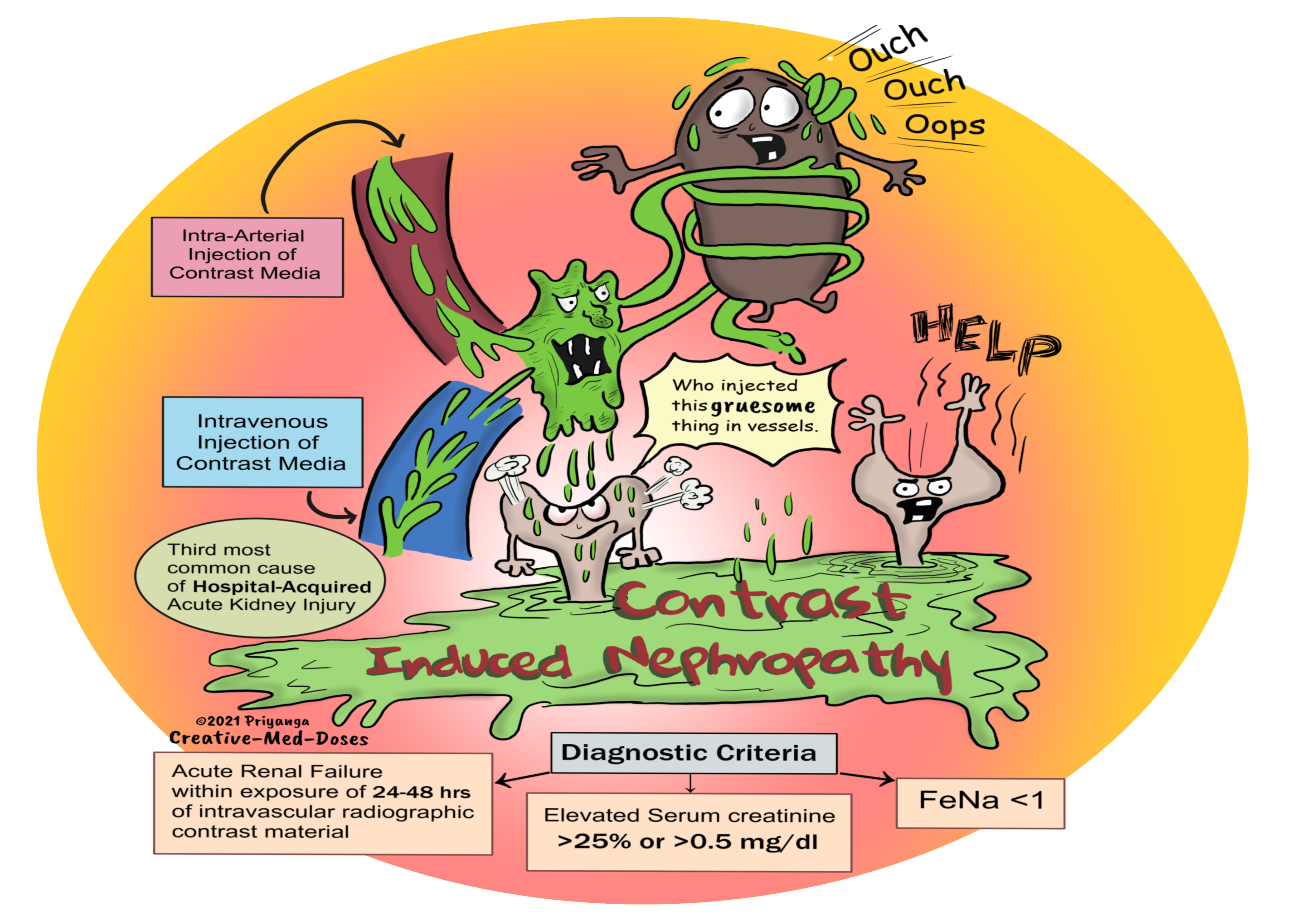
Contrast-induced nephropathy is an acute renal failure occurring within 24-48 hours of exposure to intravascular radiographic contrast material not related to other causes.
It is the third most common cause of hospital-acquired acute renal injury. The first and second causes are surgery and hypotension, respectively.
...
...
Diagnostic criteria-
- Rise in serum creatinine (Scr) levels of more than 25% or ≥0.5 mg/dl (44 μmol/l) from baseline within 48 h of contrast media exposure with the exclusion of other causes of acute kidney injury
- Signs of acute tubular necrosis
- Fractional excretion of sodium (FeNA) less than 1
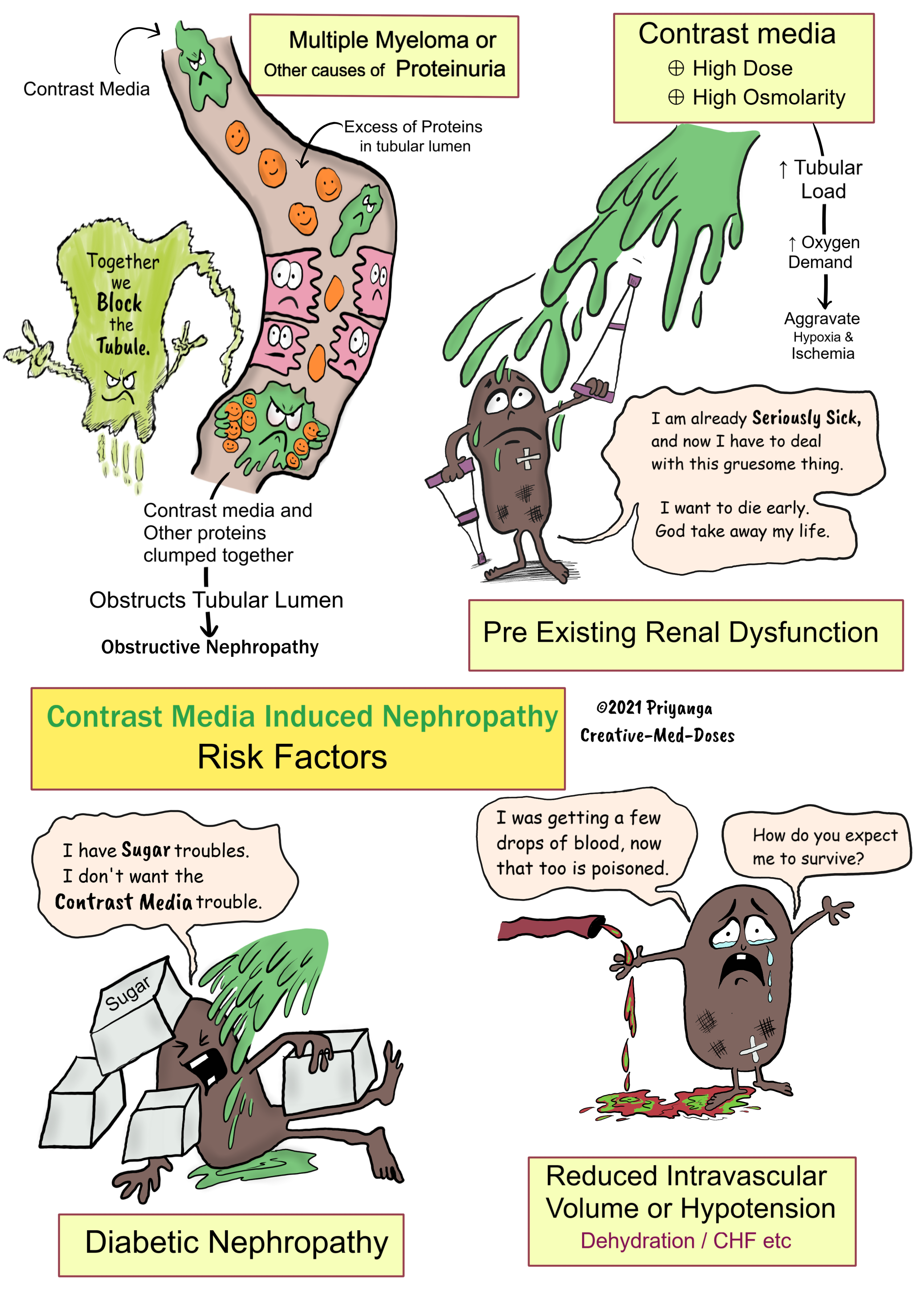
Risk factors
- Chronic Kidney Disease or preexisting impairment of renal function is the most common risk factor.
- Diabetic nephropathy
- Proteinuria- the excess protein in the tubular lumen accumulates with contrast media and causes tubular obstruction. Hypoalbuminemia increases free drug concentration in the blood which increases the risk of nephrotoxicity. (clue: most drugs are bound to albumin).
- Multiple Myeloma -It has high amounts of protein in the tubular lumen. The concomitant use of contrast material causes the accumulation of precipitated contrast media and myeloma protein in the tubular lumen. This accumulated protein, contrast media, and desquamated apoptotic tubular cells together cause tubular obstruction and acute tubular injury (obstructive nephropathy).
- Reduced intravascular volume (congestive heart failure, liver cirrhosis, or abnormal fluid losses) causes prolonged hypotension. It contributes to a prerenal reduction in renal perfusion.
- High Osmolality Contrast Media
- Amount of contrast Media
....
....
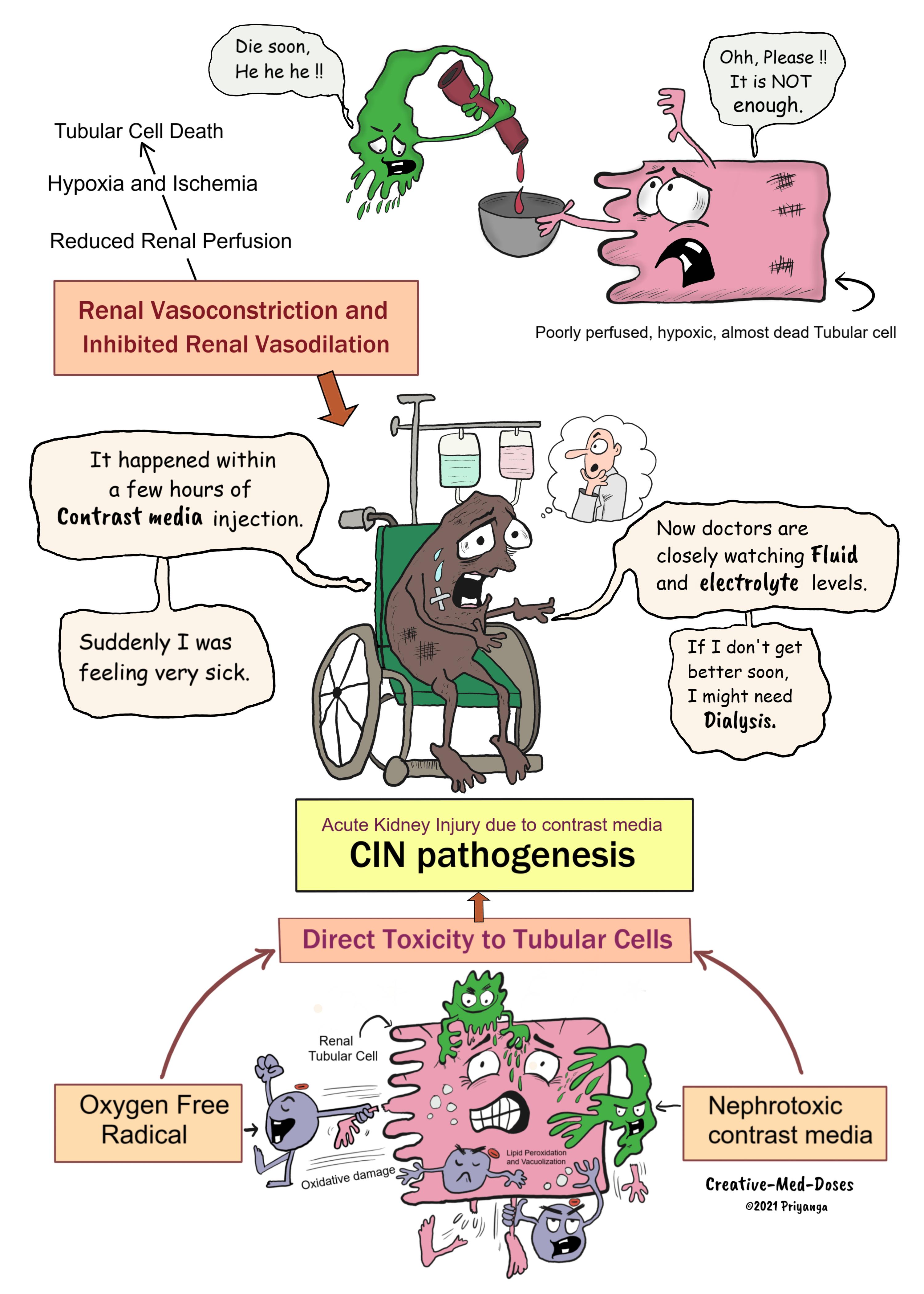
Pathophysiology of CIN
Contrast media causes acute tubular necrosis. Three pathways lead to CIN-
- Contrast media causes renal vasoconstriction and inhibition of local vasodilation (Reduced nitric oxide-mediated vasodilation). It leads to reduced renal perfusion tubular ischemia, and cell death.
- Damage by reactive oxygen species (ROS) and free radicals. The vacuolization and lipid peroxidation of tubular cells. Tubular cell injury and death.
- Direct toxicity by contrast media causes tubular cell damage and death.
...
....
Clinical Features
History of intravascular contrast media exposure within 24-48 hours.
Contrast-induced nephropathy most commonly manifests as a non-oliguric and asymptomatic transient decline in renal function.
The serum creatinine levels rise within 24 hours of contrast media administration. It usually peaks within 3–5 days and returns to normal levels within 1-2 weeks.
Oliguric acute renal failure requiring hemodialysis can also occur but is rare.
Muddy brown cast and epithelial cells are present in urinalysis.
Treatment –
- It is similar to acute kidney injury from other causes.
- Mainly supportive- Fluid and electrolyte management is crucial.
- Some cases may need Dialysis.
Prevention of CIN by-
-
- using decreased doses of contrast media
- avoiding nephrotoxic medications and volume depletion
- intravenous isotonic fluids to maintain volume
- Closely monitor renal function in a high-risk group before and once daily for five days after the radiographic procedure with contrast media exposure.
- Regularly monitoring electrolytes, BUN, and creatinine to diagnose CIN early in the course of the disease.
Buy the Nephrology book from Creative Med Doses
High-Yield Nephro Thingies
The book covers almost all high-yielding topics in nephrology.
It will be a great addition to your reading and teaching arsenal. It features cartoons, comics, and visual maps that supplement nephrology learning with relevant theory.
for the United States https://a.co/d/dus2n7d
for UK https://amzn.eu/d/jbSjqFy
Revision for today Bronchiectasis - Creative Med Doses Bronchiectasis
Read my recent books Books - Creative Med Doses