Anthrax Part 3
Hi brainy folks, last part of Bacillus Anthrax...hope you like it.
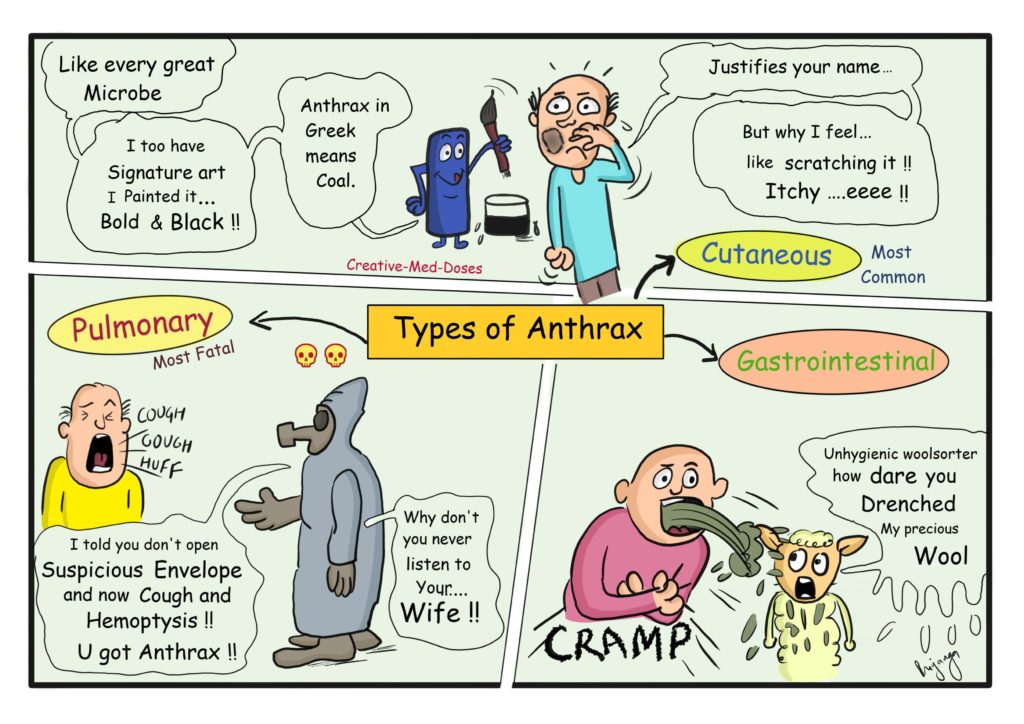
Anthrax clinical types
Cutaneous Anthrax
Most common type, mode of transmission is contact with spores and its entry through breach in skin.
Painless Pruritic Papule, which progresses into necrotic Black Eschar. Black eschar sloughs off in two weeks.
Treatment: Combination therapy (antibiotics oral + monoclonal antibody + post exposure vaccine)
Pulmonary Anthrax
Most lethal type, mode of transmission is inhalation, can complicate cutaneous anthrax into pulmonary with hematogenous spread.
Flu like symptoms with non-productive cough and hemoptysis.
ARDS (acute respiratory distress syndrome), pulmonary edema, pleural effusion
Fever, chest pain and widened mediastinum.
Treatment: Combination therapy (antibiotics oral + monoclonal antibody + post exposure vaccine)
Gastrointestinal Anthrax
Nausea, vomiting, abdominal cramp and dysentery
Treatment: Combination therapy (antibiotics oral + monoclonal antibody + post exposure vaccine)
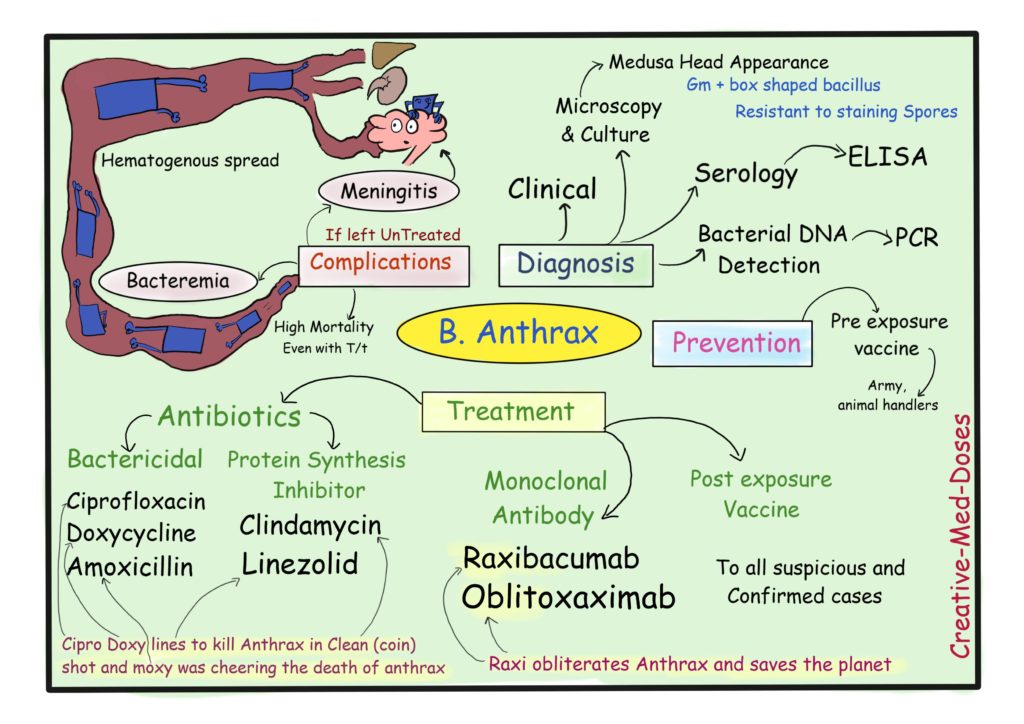
Complications
Bacteremia and meningitis
Most common in inhalational anthrax. Hematogenous spread of B. anthrax if left untreated. When it reaches to CNS it causes life threatening Meningitis.
Treatment: Combination therapy (three antibiotics IV + monoclonal antibody + post exposure vaccine)
Prognosis
Cutaneous has good prognosis if treated on time.
Pulmonary anthrax has poor prognosis and high mortality rate, sometimes even with treatment. Complication rate is higher and treatment failure is a possibility.
You can read more on anthrax here https://creativemeddoses.com/topics-list/anthrax-and-biowar/