Acute intestinal obstruction: Pathophysiology
Acute intestinal obstruction occurs either mechanically from blockage or functionally from intestinal dysmotility when there is no blockage.
Acute intestinal obstruction accounts for ~1–3% of all hospitalizations and a quarter of all urgent or emergent general surgery admissions. Approximately 80% of cases presents with the small bowel obstruction, and 1/3rd of these patients has significant ischemia. The mortality rate for patients with strangulation who are operated on within 24–30 h of the onset of symptoms is nearly 8% but increases exponentially as the time passes.
Causes
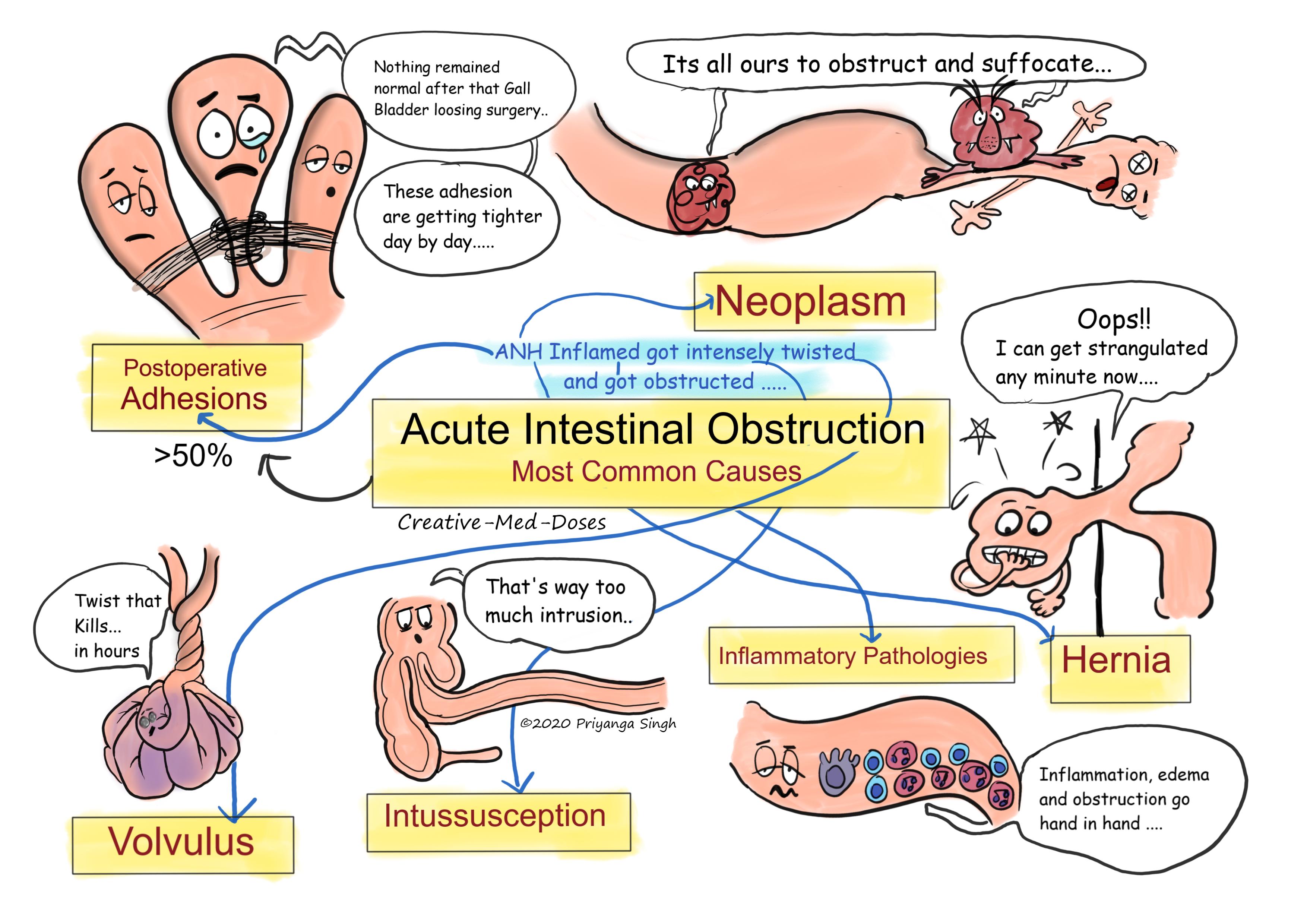
Most common causes of intestinal obstruction
• Postoperative adhesions - > 50 percent incidence
• Neoplasms- >20 percent (extrinsic or intrinsic obstruction) incidence
• Hernias - > 10 percent incidence
• Inflammatory bowel disease, other inflammation of intestine – 5 percent incidence
• Intussusception, volvulus, other miscellaneous diseases- < 15 percent
(reference Harrison 20th edition chapter 323)
...
...
Pathophysiology
Following are sequence of events in intestinal obstructions of all kinds. Closed loop obstruction tends to have faster deterioration and early strangulation and perforation. Strangulation means vascular insufficiency along with intestinal obstruction.
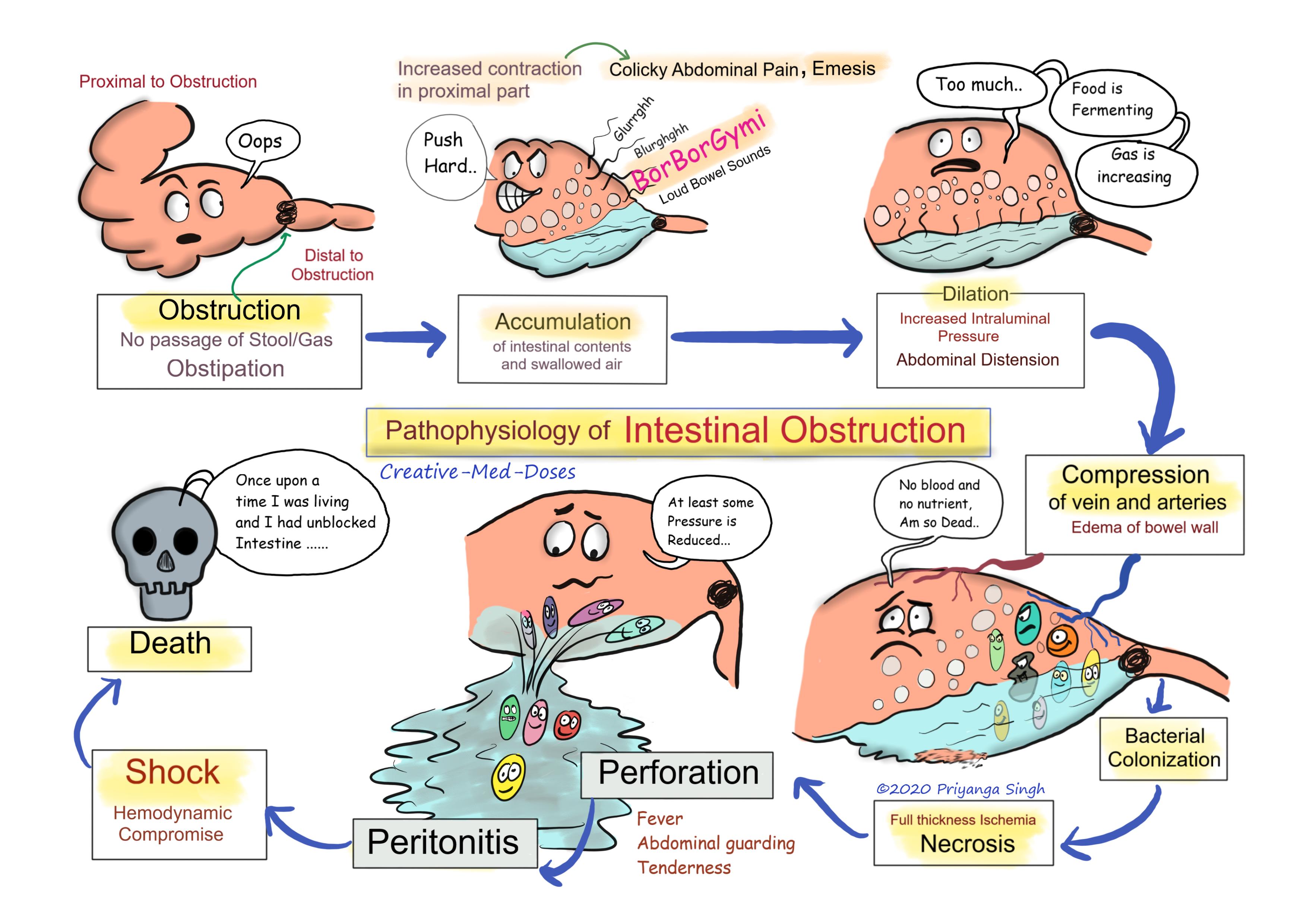
Obstruction – as soon as the intestinal obstruction occurs the distal segment of intestine collapses and proximal segment has increased intestinal contractility. This increased intestinal contractility along with accumulation of fluid and swallowed air leads to loud intestinal sound which are also called “Borborygmi”. Intestinal sounds reduce with time as the distension increases. Patients do not pass stool or gas (Obstipation).
Dilation of proximal segment- intestinal segment Proximal to obstruction has increased accumulation of intestinal content and swallowed air. With passing time, the intestinal content starts to ferment and amount of gas increases. Accumulation of fluid and air causes dilation of proximal segment and abdominal distention. This can be appreciated as air and fluid levels in abdominal radiogram of the patient. Small intestinal obstruction characteristically shows ladder pattern in abdominal X ray.
Emesis – increase accumulation of fluid and obstruction leads to increased intraluminal pressure. Increased pressure leads to bilious vomiting and loss of Hydrogen, potassium, and chloride ion in vomitus. Feculent vomiting is indicative of bacterial growth in proximal segment. Proximal obstruction has more severe and early onset of vomiting in comparison of distal bowel obstruction (for example small bowel obstruction has more severe and early vomiting than large bowel obstruction).
Compression of vessels – increased intraluminal pressure in proximal segment leads to compression of venous and arterial circulation. Venous compression causes impeded venous drainage leading to stasis and edema of bowel wall.
Full thickness Ischemia – obstruction in arterial circulation leads to full thickness ischemia of bowel wall.
Bacterial growth- combination of stasis and ischemia leads to bacterial overgrowth. It caused severe inflammation, release of inflammatory mediators and increased Gas production.
Necrosis and edema of intestinal wall- ischemia and inflammation leads to epithelial necrosis and edema of intestinal epithelium in proximal segment.
Perforation – necrosis can lead to perforation and leakage of intestinal content along with intestinal bacteria and inflammatory mediators in peritoneal cavity.
Peritonitis – the intestinal content, bacteria and inflammatory mediators causes peritoneal irritation and peritonitis. Patient has fever, abdominal tenderness and guarding. Emergency surgery is required to save life.
Shock- if immediate interventions are not started patient’s condition deteriorate exponentially leading to hemodynamic compromise, hypotension, oliguria, and tachycardia.
Death – intestinal obstruction cases with perforation and shock may die if not attended immediately.
...
...
Case scenario
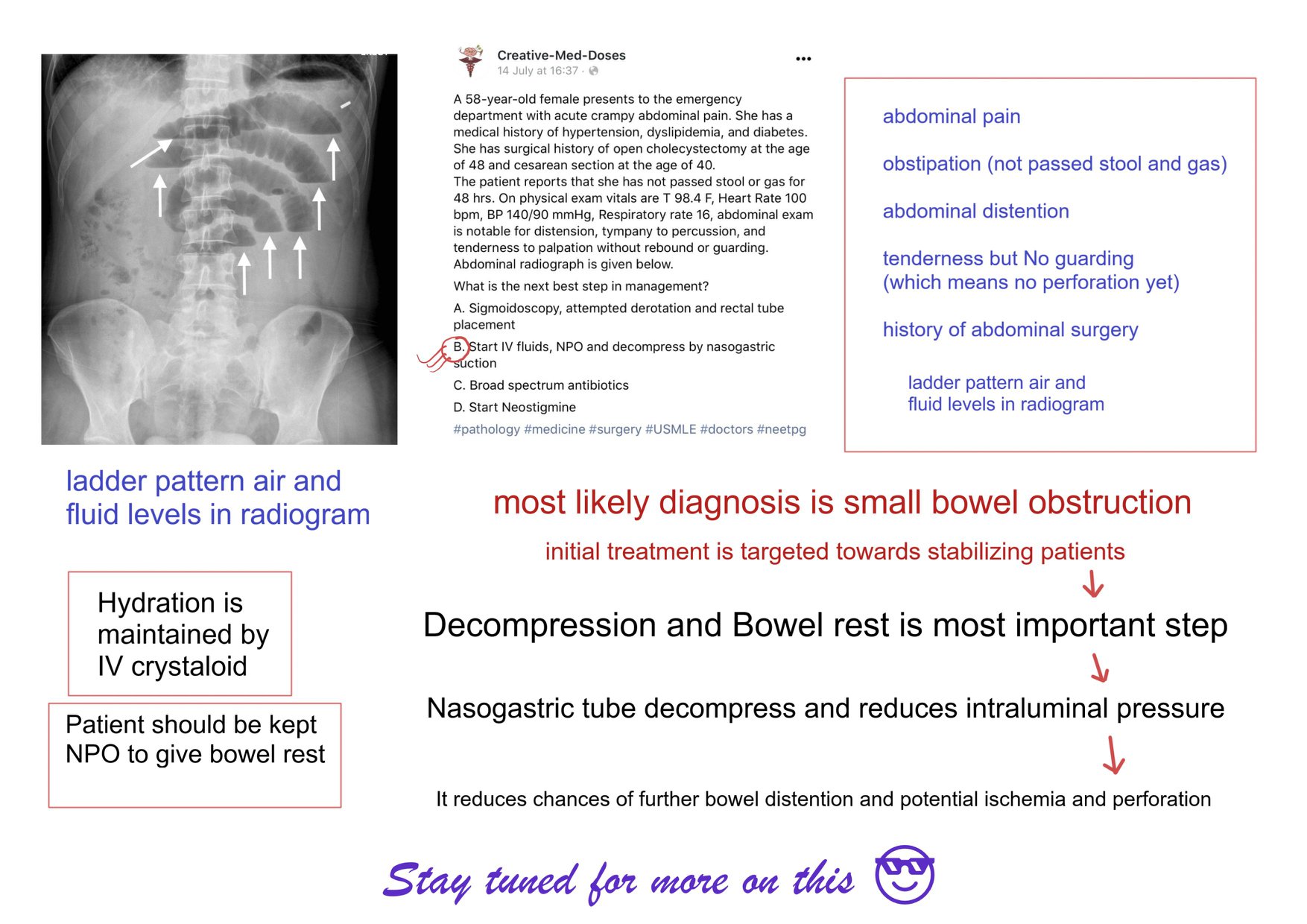
A 58-year-old female presents to the emergency department with acute crampy abdominal pain. She has a medical history of hypertension, dyslipidemia, and diabetes. She has surgical history of open cholecystectomy at the age of 48 and cesarean section at the age of 40.
The patient reports that she has not passed stool or gas for 48 hrs. On physical exam vitals are T 98.4 F, Heart Rate 100 bpm, BP 140/90 mmHg, Respiratory rate 16, abdominal exam is notable for distension, tympany to percussion, and tenderness to palpation without rebound or guarding.
Abdominal radiograph is given below.
What is the next best step in management?
- Sigmoidoscopy, attempted derotation and rectal tube placement
- Start IV fluids, NPO and decompress by nasogastric suction
- Broad spectrum antibiotics
- Start Neostigmine
Answer is 2
...
...
Revision for today is Erb's Palsy
Buy fun review books here (these are kindle eBook’s you can download kindle on any digital device and login with Amazon accounts to read them). Have fun and please leave review.
Subscribe YouTube channel Creative-Med-Doses