Tetralogy of Fallot: Fatal Four
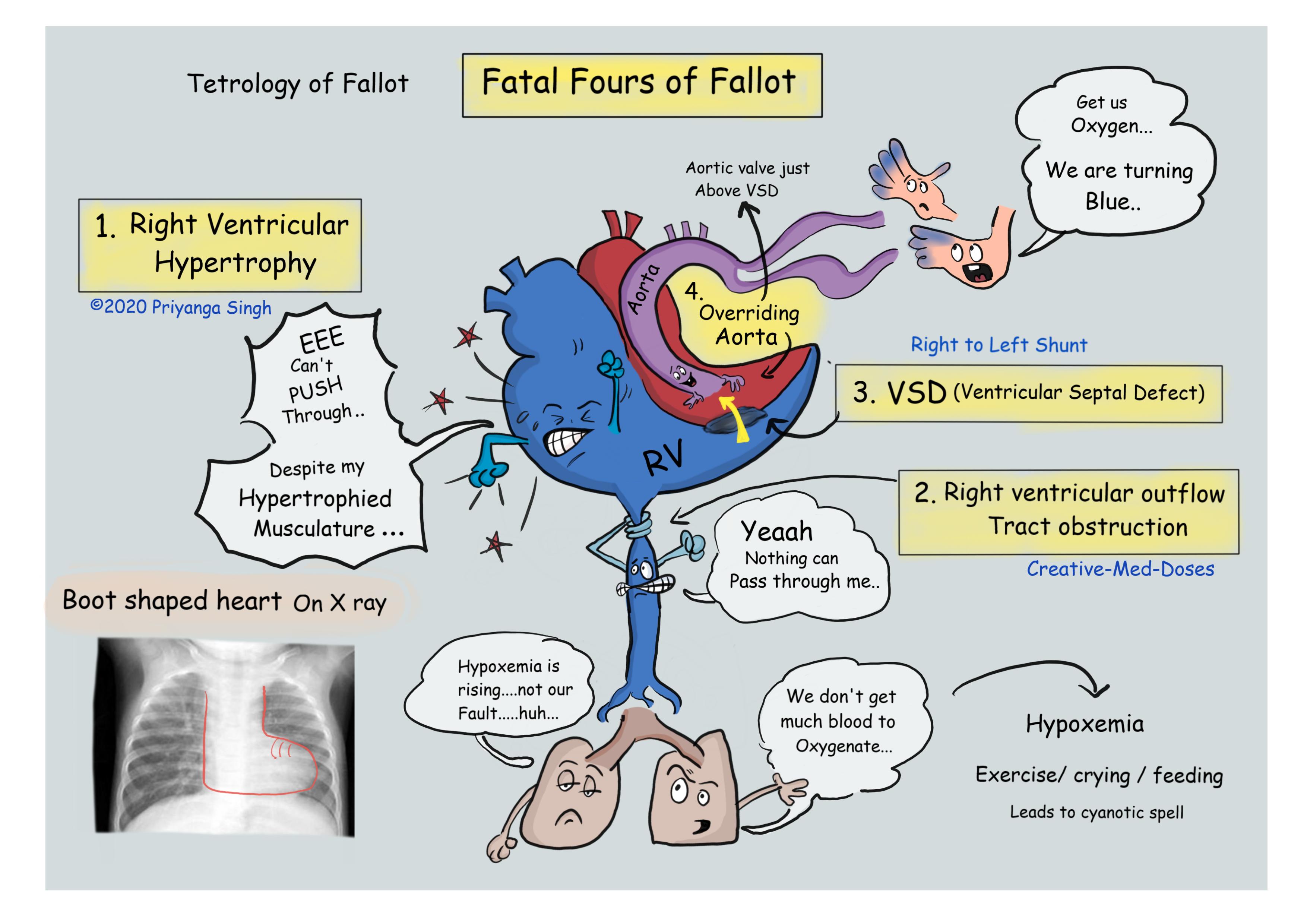
Tetralogy of Fallot is a congenital cardiac defect caused by anterosuperior displacement of the infundibular septum, characterized by four defects occurring together-
- Right ventricular outflow tract obstruction (subpulmonic stenosis)
- Ventricular septal defect (VSD)
- Overriding of the VSD by the aorta
- Right ventricular hypertrophy (RVH)
Pathophysiology
Conotruncal abnormality from failure of neural crest cells to migrate. All the features of tetralogy of Fallot result from anterosuperior displacement of the infundibular septum leading to abnormal septation between the pulmonary trunk and the aortic root.
- Right ventricular hypertrophy (RVH): Narrowing or blockage of the pulmonary valve or infundibulum causes restriction of blood outflow. This leads to increase in right ventricular work and pressure, leading to right ventricular thickening or hypertrophy.
- Ventricular septal defect (VSD): There is a hole in the ventricular septum of child’s heart. The oxygen-poor blood in the right ventricle gets mixed with oxygen-rich blood in the left ventricle because of this septal defect. This poorly oxygenated blood is then pumped out of the left ventricle to the rest of the body. Hypoxemia causes cyanosis giving bluish color to the skin, lips, and membranes inside the mouth and nose.
- Overriding of the VSD by the aorta: the aortic valve is situated immediately over the VSD also called overriding aorta. It is the main site for outflow of blood from both ventricles.
- Right ventricular outflow tract obstruction (pulmonary stenosis): The major issue and most important prognostic factor in tetralogy of Fallot is the degree of pulmonary valve stenosis. If the stenosis is mild, there is low pressure in right ventricle and thus left to right shunt is present, minimal cyanosis occurs, since blood still mostly travels to the lungs. However, if the PS is moderate to severe, right ventricle has very high pressure leading to right to left shunt and a smaller amount of blood reaches the lungs, most is shunted right-to-left through the VSD. It causes significant hypoxemia and cyanosis.
...
...
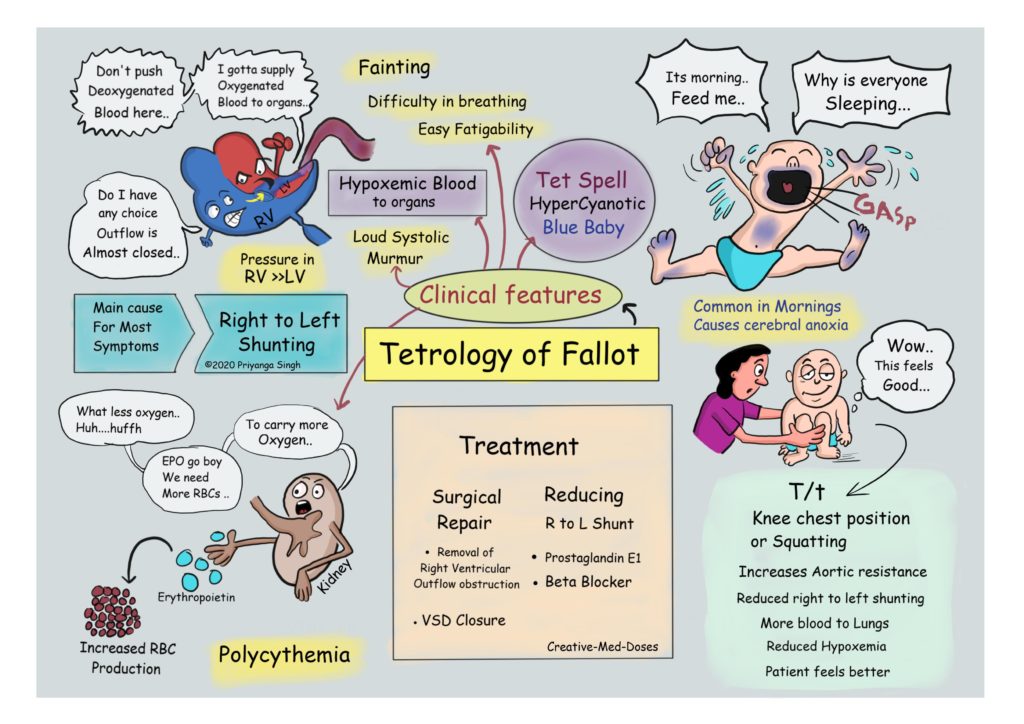
Clinical features
The clinical severity largely depends on the degree of the pulmonary outflow obstruction, it is the most important prognostic factor.
- Tet spells (hyper cyanotic episodes) -- Episodes of extreme blue coloring. In this child suddenly becomes blue, has difficulty breathing, and may become extremely irritable or even faint. Tet spells are caused by crying, fever, or any physical exertion, it often resolves with knee-chest position/ squatting position or oxygen.
- Fainting and Troubled breathing
- Easy fatigues, growth retardation
- Clubbing (in older children with uncorrected defect)
- Loud and harsh systolic ejection murmur on the upper sternal border
- Hypertrophic osteoarthropathy
- Polycythemia (due to hypoxia)
- Infective endocarditis and systemic embolization
Diagnosis
- On basis of clinical presentation
- Echocardiogram shows VSD and other features of Tetrology of fallout.
- Radiological images show “boot shaped heart” due to right ventricular hypertrophy.
...
...
Treatment
- Prostaglandin E1 and β-blockers to reduce frequency of hyper cyanotic episodes.
- Surgical repair of pulmonary stenosis and closure of VSD.
Case Scenario
A 5-month infant presents with his mother to pediatrician for episodes of turning blue while crying. The mother reports that his lips turn blue when he is crying or being fed, he typically gets better after knee-chest position. On physical exam, the infant is underweight and shows delayed milestones. Cardiac exam reveals a harsh systolic ejection murmur. A chest radiograph is performed and demonstrates a "boot-shaped" heart.
What is most likely diagnosis? Explain boot shaped heart??
Further reading https://casereports.onlinejacc.org/content/1/4/523.full
Must watch video https://www.youtube.com/watch?time_continue=60&v=8BJOUfycsxo&feature=emb_logo
Revision for today https://creativemeddoses.com/topics-list/digeorge-syndrome-thymic-aplasia/