Renal cell carcinoma (RCC)
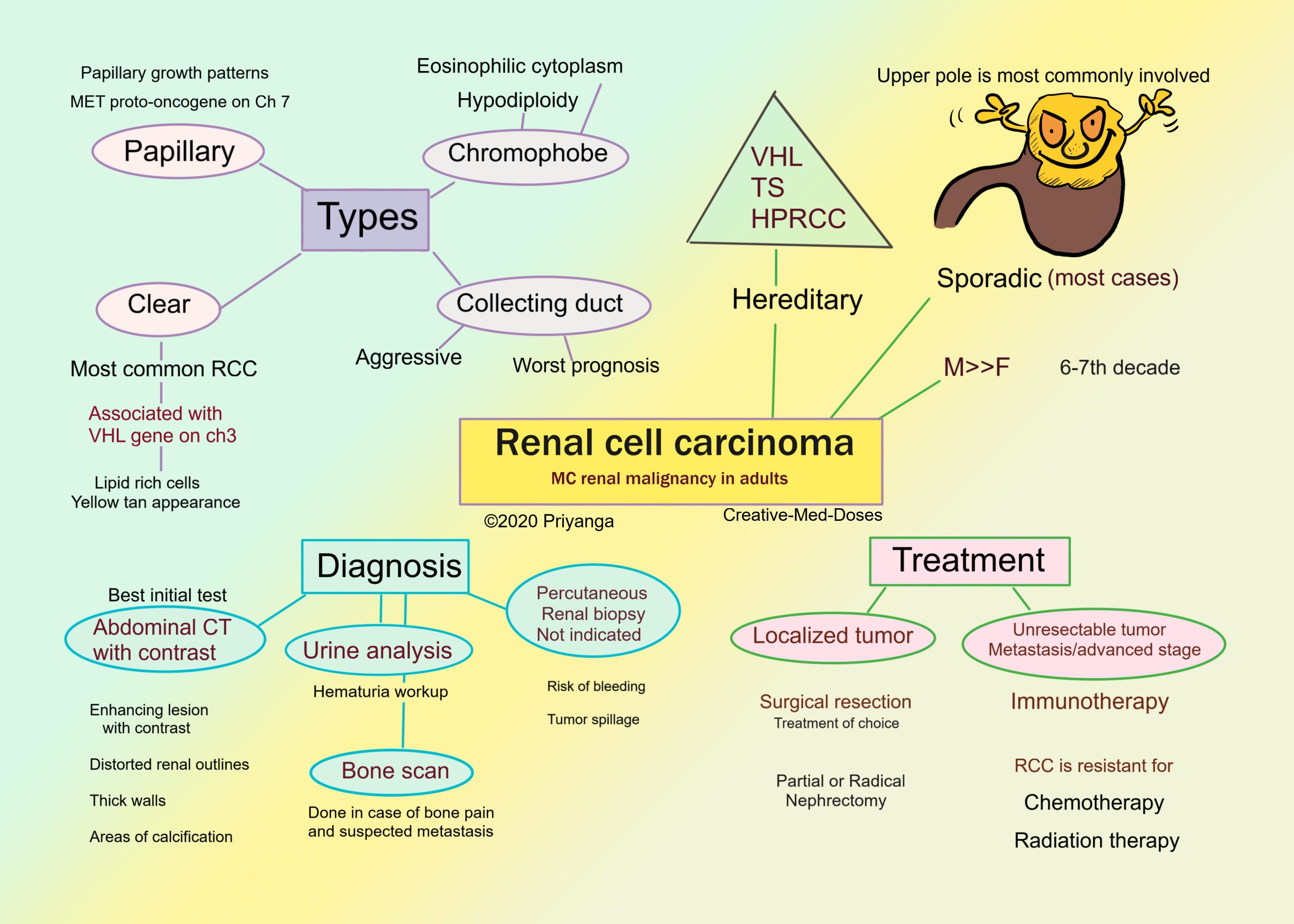
Renal cell carcinoma (RCC) arises from the renal tubular epithelium. It is the most common renal malignancy in adults (nearly 85% of renal cancers are RCC). RCC can be sporadic (in most cases) or associated with hereditary disorders.
Age on onset 6th -7th decade, more common in man. Hereditary renal cell carcinomas have an early age of onset.
High-risk group
- Smokers
- Hypertensive
- Obese
- Genetic factors
- The acquired polycystic disease-The risk for developing renal cell cancer is increased 30-fold in individuals with the acquired polycystic disease.
Hereditary RCCs are associated with-
- von Hippel-Lindau
- tuberous sclerosis
- hereditary papillary renal cell carcinoma (HPRCC)
Types
Clear cell carcinoma
- the most common form of RCC. It is associated with homozygous loss or inactivation of the VHL tumor suppressor protein.
- solitary and unilateral
- polygonal cells with a clear, glycogen, and lipid-filled cytoplasm. They are arranged as cords or tubules. They have a clear appearance under the microscope because lipids and carbohydrates are washed away in routine H&E staining, leaving empty clear cells.
- the cut surface is yellow to orange due to the high lipid content of cells. Necrosis, hemorrhage, and cystic degeneration are also present.
Papillary carcinoma
- 10% to 15% of all renal cancers
- papillary growth pattern with fibrovascular cores.
- cut surface shows necrosis, hemorrhage, and cystic degeneration.
- frequently multifocal and bilateral
- hereditary papillary RCC is associated with the MET proto-oncogene on chromosome 7q.
Chromophobe carcinoma
- 5% of all renal cell carcinomas
- arise from intercalated cells of collecting ducts.
- large polygonal cells with eosinophilic cytoplasm and a perinuclear halo.
- multiple losses of entire chromosomes cause extreme hypodiploidy.
Collecting duct carcinoma
- arise from Medullary collecting duct
- malignant glandular cells arranged in an irregular pattern within a fibrous stroma (hobnail pattern)
- aggressive tumors with poor prognosis
Clinical Features
Renal cell carcinomas are asymptomatic in the early stages (silent tumors). The large tumors (>10 cm) or metastasized tumors become symptomatic.
The classical triad of RCC consists of the following-
- Hematuria-- the most frequent presenting manifestation (> 50% of cases). Macroscopic hematuria tends to be intermittent and fleeting, superimposed on steady microscopic hematuria. When the tumor invades the collecting system, it causes hematuria.
- Flank pain and colicky abdominal pain
- Palpable mass-- Firm, nontender, and homogeneous on palpation
Fever and weight loss are constitutional symptoms.
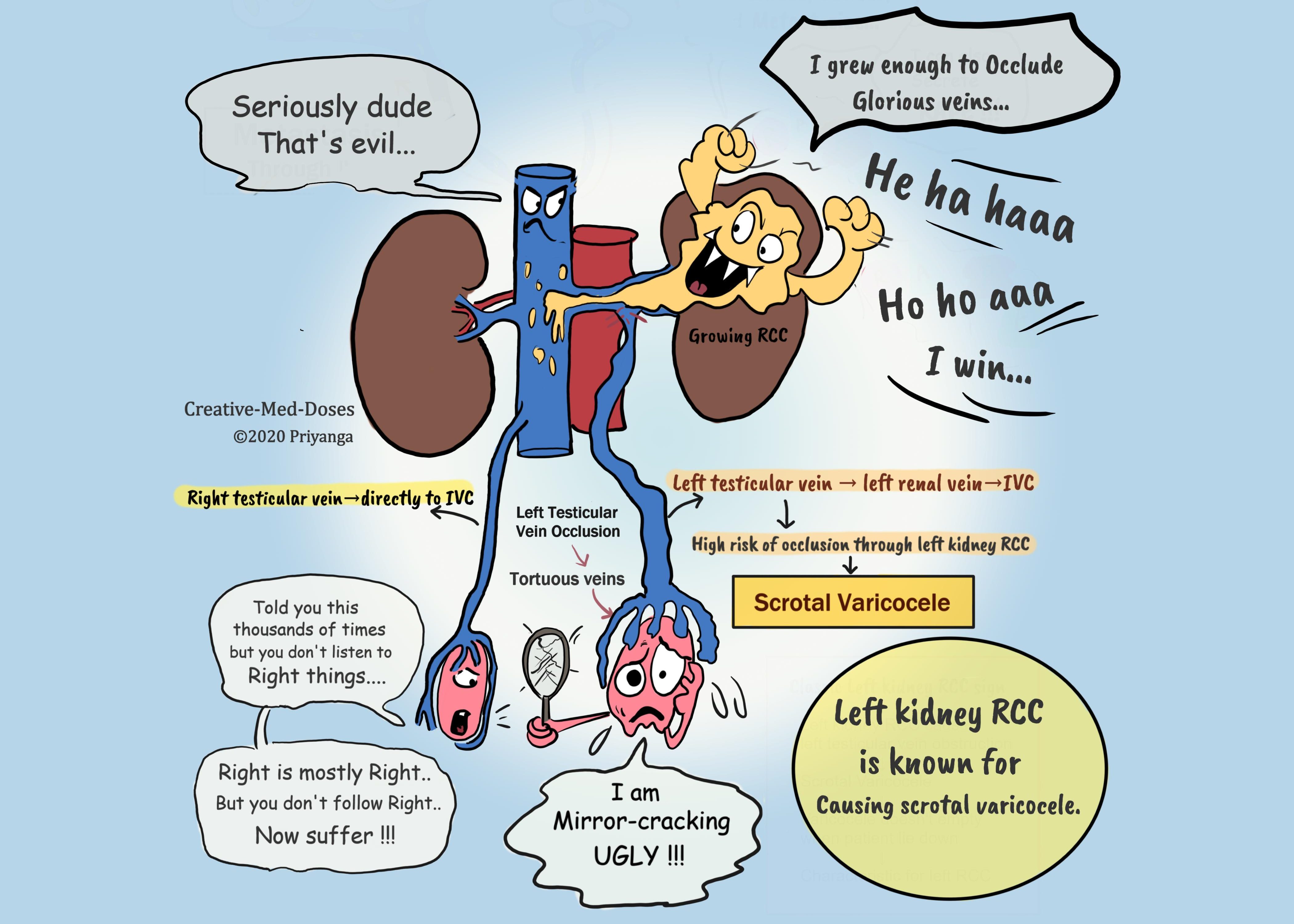
Scrotal varicocele
The varicocele in male patients, which does not empty when the patient lies down, is the classic sign of left kidney RCC. The left testicular vein drains in the left renal vein before draining into the inferior vena cava (IVC). The left testicular vein gets occluded by the growing RCC at the point where it joins the left renal vein. The blocked venous drainage makes scrotal veins engorged and dilated → scrotal varicocele.
The right testicular vein drains directly into IVC, which is why chances of right testicular vein occlusion by tumor are much lesser.
Signs and symptoms of IVC obstruction and invasion
- Ascites
- Lower extremity swelling (edema)
- Pulmonary emboli
- Hepatic dysfunction
...
...
Paraneoplastic syndromes
The tumor cells secrete various hormones, and this ectopic secretion causes different signs and symptoms related to a particular hormone-
Renin secretion causes hypertension
ACTH (Adreno-cortico tropic hormone) causes increased cortisol
PTHrP (parathyroid hormone-related peptide) causes hypercalcemia
EPO (erythropoietin) causes polycythemia
Diagnosis
Best initial test: abdominal CT scan with contrast
- enhancing lesion with contrast
- thickened irregular walls or septa
- distorted renal outline and stretched renal calyces
- areas of necrosis and calcification
Urinalysis – for hematuria
Bone scan – in case of bone pain and suspected metastasis into bones.
Percutaneous renal biopsy is not advised because of the increased chances of tumor seeding and bleeding.
Treatment
Surgical resection of the tumor and involved area is the treatment of choice.
Localized tumor
- Nephrectomy--Partial or Radical nephrectomy
Unresectable tumors (metastasis and locally advanced)
- Systemic treatment— Immunotherapy
...
...
Prognosis
Tumors diagnosed at the early stages with limited spread have a good prognosis.
- Sarcomatoid changes in any form of RCC has the worst prognosis.
- Collecting duct carcinomas also have a poor prognosis.
Case scenario
A 64-year-old male presents to the physician for abdominal discomfort and hematuria. The patient states he first noticed pain on his right flank a few months ago, and it is gradually increasing in intensity. The patient gives no history of fever, chills, and dysuria. Physical examination reveals a palpable mass in the left flank. He is a chronic smoker and known hypertensive. His CBC reveals a hemoglobin of 18 and hematocrit of 53%. The urinalysis is positive for red blood cells and negative for leukocytes. Which of the following is the most likely diagnosis?
- Aortic aneurysm
- Polycystic kidney disease
- Pyelonephritis
- Renal cell carcinoma
Revision for today Potter’s Sequence - Creative Med Dosehttps://creativemeddoses.com/topics-list/potters-sequence/
Buy books here Books - Creative Med Doses