Pulmonary Hypertension
Pulmonary hypertension is defined as an elevation in mean pulmonary artery pressure (PAP) > 20 mm Hg or more at rest. Normal PAP levels are 8-20 mmHg.
Hemodynamic definition PH vs PAH
Pulmonary hypertension (PH) = mPAP > 20 mm of Hg at rest
Pulmonary Arterial Hypertension (PAH) has mPAP of >20 mm of Hg at rest but it has Pulmonary capillary wedge pressure (PCWP) <15 mm of Hg (normal PCWP).
Right heart catheterization is the gold standard test for pulmonary artery pressure measurement.
Classification
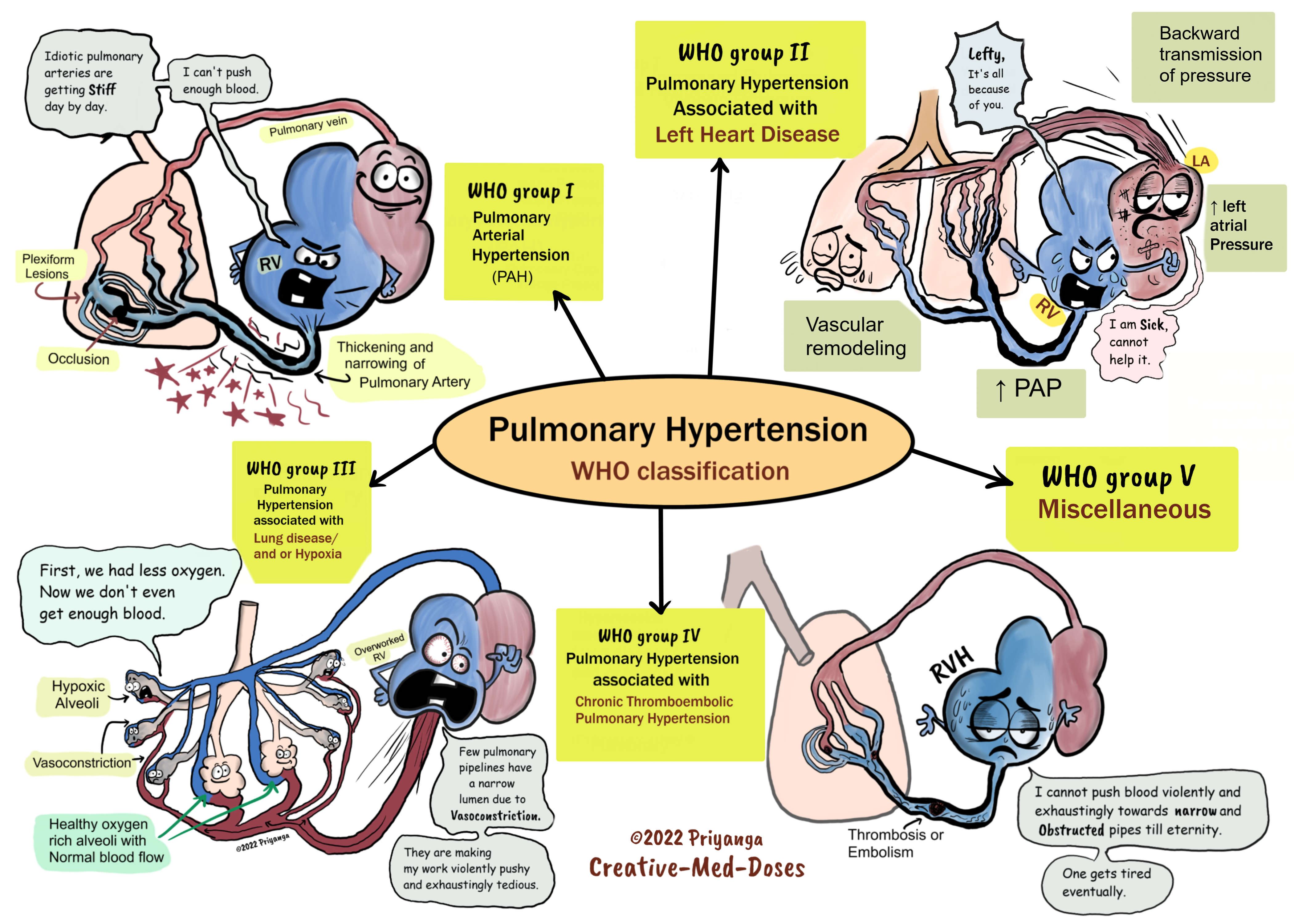
Pulmonary hypertension is classified into five groups by the World Health Organization (WHO)-
- Pulmonary arterial hypertension (PAH) is associated with heritable forms of pulmonary hypertension and diseases that cause pulmonary hypertension by affecting small pulmonary muscular arterioles. These include connective tissue diseases, human immunodeficiency virus, and congenital heart disease with a left to right shunt
- Pulmonary hypertension due to left-sided heart disease, including systolic and diastolic dysfunction and valvular disease
- Pulmonary hypertension due to lung diseases and/or hypoxia, including COPD and interstitial lung disease
- Chronic thromboembolic pulmonary hypertension (CTEPH)
- Pulmonary hypertension with unclear or multifactorial mechanisms
....
....
Pathogenesis
Most common causes associated with PH-
- Chronic obstructive or interstitial lung diseases-
These diseases obliterate alveolar capillaries, increase pulmonary vascular resistance, and elevate the pulmonary blood pressure.
Hypoxia is a potent stimulus for vasoconstriction in the pulmonary circulation. The hypoxic alveoli get less blood due to vasoconstriction in supplying vessels, and the blood diverts to oxygen-rich alveoli. The hypoxic vasoconstriction is a homeostasis mechanism to maintain ventilation/ perfusion match.
Chronic hypoxia (COPD / High Altitude) causes persistent vasoconstriction and increases peripheral vascular resistance and pulmonary hypertension.
- Congenital or acquired heart disease.
Left-to-right shunts present in ASDs, VSDs, and PDA result in increased Right ventricular cardiac output and pulmonary vascular congestion. Increased pulmonary blood flow leads to shear and circumferential stress triggering vascular remodeling. The vascular remodeling includes increased endothelial proliferation, intimal fibrosis, and smooth muscle cell proliferation. It leads to vascular lumen narrowing and thickened resistant pulmonary vessel wall that increases the pulmonary vascular resistance.
Mitral stenosis causes an increase in left atrial pressure and pulmonary venous pressure. The increase in pulmonary venous pressure is transmitted to the pulmonary artery and its branches causing pulmonary hypertension.
- Recurrent thrombo-emboli.
Recurrent pulmonary emboli cause obliteration and turbulence in blood flow that leads to an increase in pulmonary vascular resistance and leads to pulmonary hypertension.
- Autoimmune diseases
Autoimmune diseases like systemic sclerosis have a microvascular disease with endothelial activation, injury, and increased platelet activation. The endothelial injury and platelet aggregation in pulmonary vasculature trigger endothelial proliferation, intimal fibrosis, and perivascular fibrosis resulting in increased pulmonary vascular resistance and pulmonary hypertension.
- Obstructive sleep apnea related hypoxia leads to pulmonary vasoconstriction and subsequent increase in pulmonary vascular resistance and pulmonary hypertension.
The pathway towards pulmonary hypertension in most cases
Disturbed/ turbulent blood flow →shear and stress cause endothelial injury → activation of multiple vascular remodeling pathways→ endothelial cells and smooth muscle proliferation and increased intimal fibrosis→ stiff and resistant vessels→ increased pulmonary vascular resistance→ increased right ventricular afterload (right ventricle has to pump harder to push blood towards pulmonary vasculature) → Right ventricular hypertrophy →Right heart failure (RHF)
Morphology
Pulmonary hypertension is associated with
- medial hypertrophy of the pulmonary muscular and elastic arteries
- pulmonary arterial atherosclerosis
- plexiform lesion- the tuft of capillary formations produces a network, or web, that spans the lumens of dilated thin-walled, small arteries and may extend outside the vessel (characteristic of Pulmonary hypertension)
- right ventricular hypertrophy
Clinical presentation
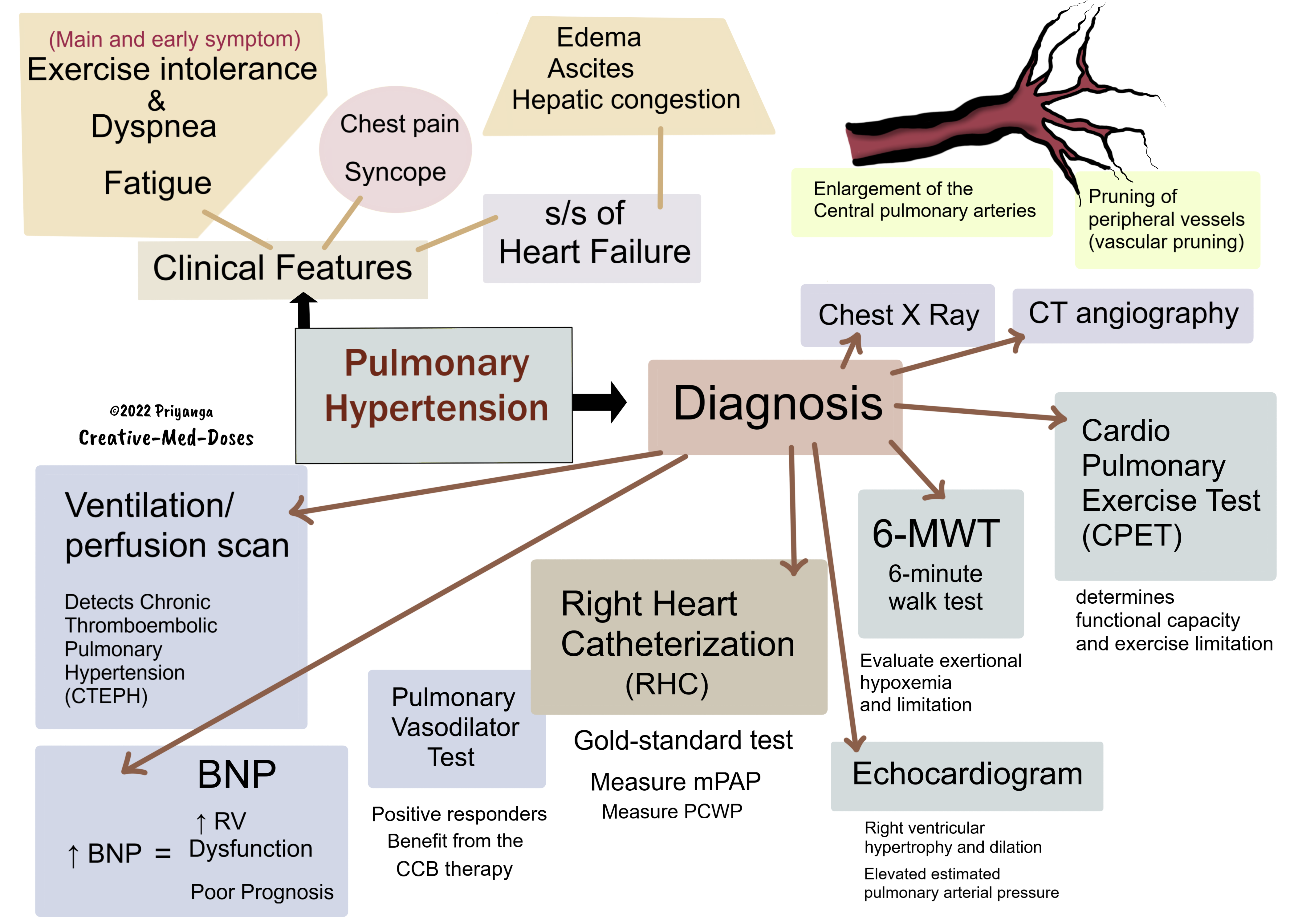
The main and early symptoms of PH are exercise intolerance and dyspnea.
- Exertional dyspnea
- Fatigue
- Exertional Chest pain / anginal chest pain
- Exercise limitation
- Syncope
- Edema, ascites
- Hepatic congestion/hepatomegaly leading to right upper quadrant pain and anorexia
Physical examination shows -
evidence of right ventricular failure -
- elevated jugular venous pressure
- lower extremity edema
- ascites
on auscultation
- accentuated P2 component of the second heart sound
- a right-sided heave due to right ventricular hypertrophy
- a holosystolic tricuspid regurgitant murmur
Diagnosis
Chest imaging
- enlargement of the central pulmonary arteries
- pruning of peripheral vessels (vascular pruning)
- cardiomegaly (right atrial and ventricular enlargement, suggestive of advanced disease)
Echocardiogram (Initial screening test)
Transthoracic Echocardiography (TTE) findings
- Right ventricular hypertrophy and dilation
- elevated estimated pulmonary arterial pressure
Cardiopulmonary Exercise Test (CPET)
The cardiopulmonary exercise test (CPET) determines functional capacity and exercise limitation in cases of pulmonary hypertension. It provides information about cardiovascular, respiratory, metabolic, and muscular responses to exercise.
It is also known as an oxygen consumption test (exercise stress test) that measures exercise ability.
Right heart catheterization (RHC)
Right heart catheterization (RHC) is the gold-standard test for measurement of pulmonary artery pressure (PAP) and diagnosis of pulmonary hypertension. It is also a useful test in the selection of appropriate medical therapy for PH.
In RHC, a thin, flexible catheter is guided into the right lower heart chamber (right ventricle) and pulmonary artery through a femoral vein/brachial vein, or internal jugular vein.
RHC differentiates PAH from Post capillary PH
RHC findings in Precapillary PH or pulmonary artery hypertension (PAH)
- Increased mean PAP (mPAP >25 mmHg)
- Normal pulmonary capillary wedge pressure (PCWP), left atrial pressure, left ventricular end-diastolic pressure (LVEDP) ≤15 mmHg
- PVR >3 Wood units
RHC findings in Post capillary PH
- Increased mean PAP (mPAP >25 mmHg)
- Increased PCWP ≥15 mmHg
RHC and Pulmonary vasodilator test
Pulmonary vasodilator testing identifies the CCB therapy responders in PAH cases.
Vasodilators can only dilate vessels with reversible vasoconstriction. The fixed or stenosed vessels do not dilate in response to vasodilators.
Short-duration vasodilators like Intravenous adenosine, intravenous Epoprostenol, inhaled nitric oxide, or inhaled Iloprost are preferred agents.
Positive vasodilator test
In cases where the numbers of reversibly vasoconstricted vessels are higher than stenosed vessels, the vasodilator will dilate the reversibly constricted pulmonary vessels, reduces the pulmonary vascular resistance, and drops the pulmonary artery pressure (PAP).
Patients with positive vasodilator response may benefit from long-term use of calcium channel blocker (CCB) therapy and have a good prognosis. A decrease in the mean pulmonary artery pressure by at least 10 mmHg to reach an absolute value of 40 mmHg or less without a decrease in cardiac output is currently considered a positive pulmonary vasodilator test.
Negative vasodilator test
In cases where the number of reversibly vasoconstricted vessels is lesser than fixed stenosed vessels, the pulmonary vascular resistance doesn’t drop, and PAP also doesn’t fall significantly. CCB therapy is not for such cases.
CT angiography
- Enlarged pulmonary arteries
- Peripheral pruning of the small vessels
BNP
Brain natriuretic peptide (BNP) and the N-terminus of its pro-peptide (NT-proBNP) correlate with right ventricular dysfunction, hemodynamic severity, and functional status in PAH.
A stressed right ventricle with increased afterload releases more BNP. Elevated BNP means more right ventricular dysfunction and severe pulmonary hypertension.
Pulmonary function tests
- Isolated reduction of Diffusing capacity of the lung for carbon monoxide (DLCO) -classic finding of PAH
- 6-minute walk test – evaluate exertional hypoxemia and limitation and monitor response to treatment.
Ventilation/perfusion scan
Detects Chronic thromboembolic pulmonary hypertension (CTEPH)
...
...
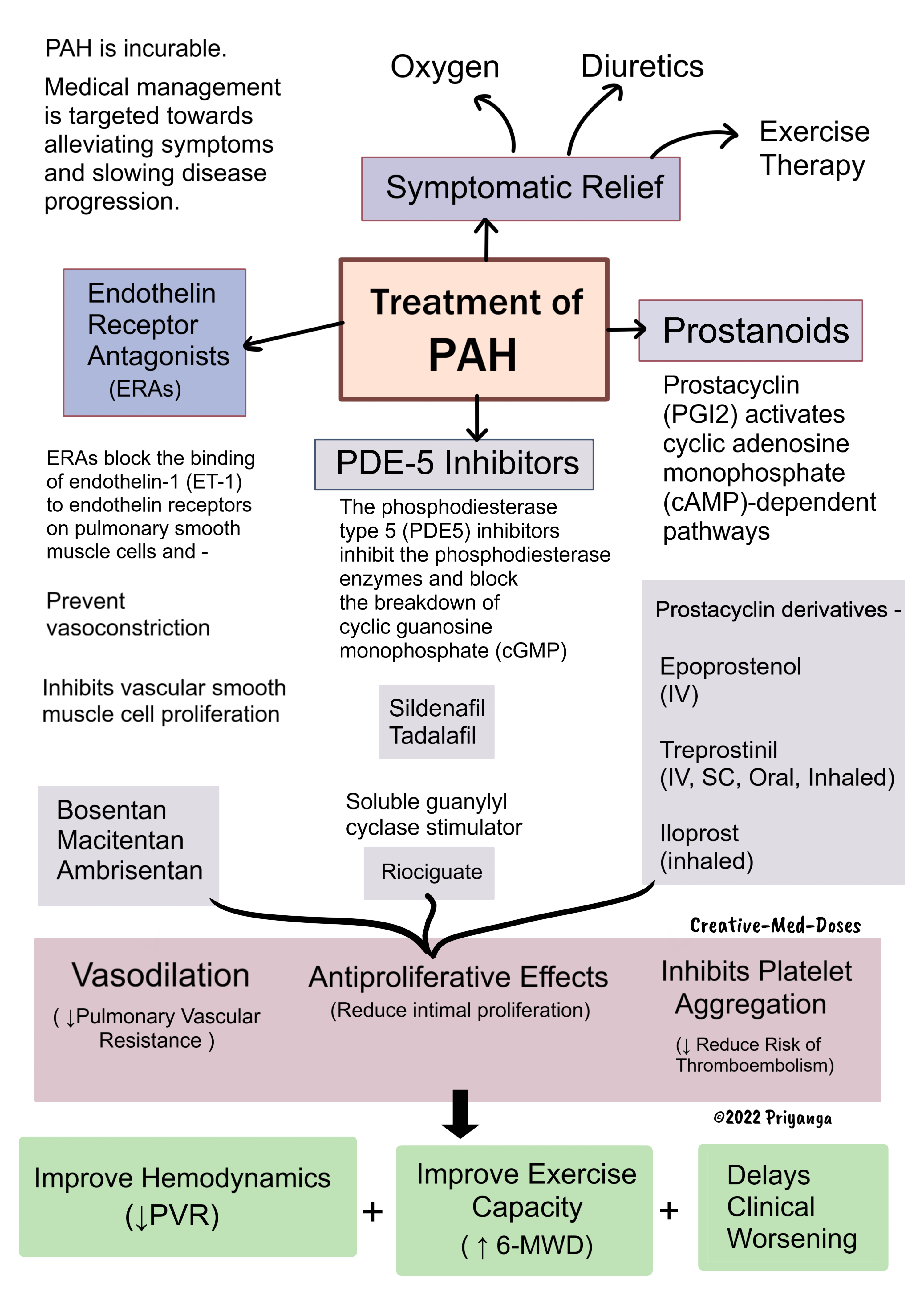
Treatment of PAH
PAH has no cure. Medical management is targeted
towards alleviating symptoms and slowing disease progression.
Pulmonary hypertension secondary to other diseases – treat the underlying cause.
Medical management
Symptomatic relief
- Oxygen
- Diuretics
- Exercise therapy
Prostanoids
Prostacyclin (PGI2) activates cyclic adenosine monophosphate (cAMP)-dependent pathways and mediates -
- Vasodilation- reduce PVR
- Antiproliferative effects on vascular smooth muscle – reduced intimal proliferation and fibrosis
- Inhibits platelet aggregation- reduces the risk of thromboembolism and pulmonary artery obstruction
Prostacyclin derivatives -
- Epoprostenol (IV)
- Treprostinil (IV, SC, Oral, Inhaled)
- Iloprost (inhaled)
Selective IP receptor agonist-
- Selexipeg (Oral)
All Prostanoids improve hemodynamics, increase 6MWD (6-minute walk distance), improves exercise capacity, and delay clinical worsening.
PDE-5 inhibitors
The phosphodiesterase type 5 (PDE5) inhibitors inhibit the phosphodiesterase enzymes and block the breakdown of cyclic guanosine monophosphate (cGMP)
Accumulation of cGMP mediates
- Vasodilation by smooth muscle cell relaxation
- Inhibition of smooth muscle proliferation
- Inhibits platelet activation
PDE-5 inhibitors used in PAH-
- Sildenafil
- Tadalafil
Riociguate is a soluble guanylyl cyclase stimulator with similar effects as the PDE-5 inhibitors.
Sildenafil, Tadalafil, and Riociguate significantly improve exercise capacity (6-MWD), pulmonary hemodynamics, and delay clinical worsening.
Endothelin Receptor Antagonists (ERAs)
ERAs block the binding of endothelin-1 (ET-1) to endothelin receptors on pulmonary smooth muscle cells and -
- Prevent vasoconstriction
- Inhibits vascular smooth muscle cell proliferation
ERAs-
- Bosentan
- Macitentan
- Ambrisentan
....
....
Revision for today Diffuse Esophageal Spasm (DES) - Creative Med Doses
Buy fun review books here (these are kindle eBook you can download kindle on any digital device and log in with Amazon accounts to read them). Have fun and please leave a review.