Polycythemia vera
Polycythemia vera (PV) is a chronic myeloproliferative disorder with trilineage proliferation (erythroid, granulocytic, megakaryocytic).
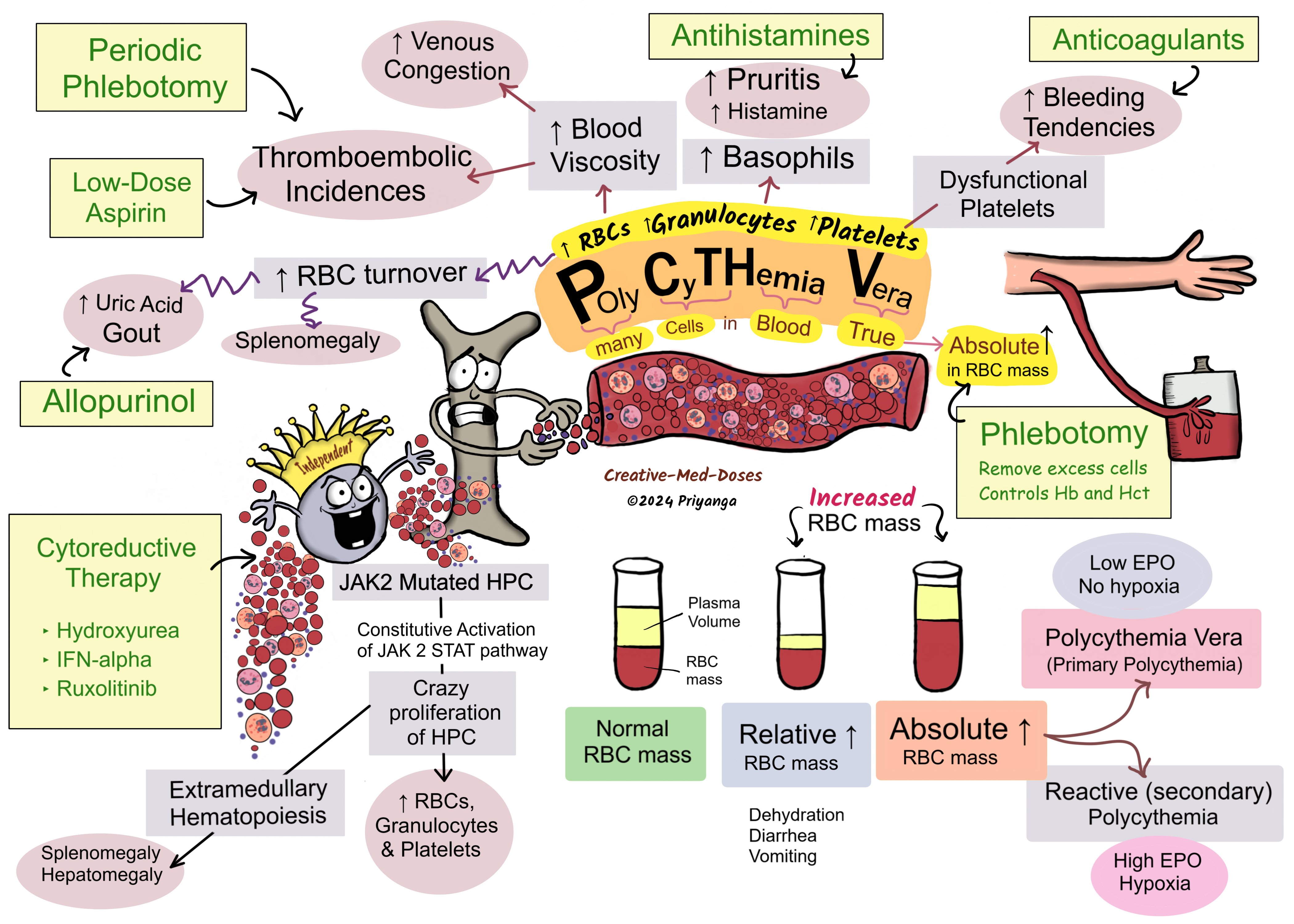
It leads to an increased number of RBCs, granulocytes (Neutrophils, basophils, and eosinophils), and Platelets.
It is associated with an absolute increase in RBC mass.
PV must be differentiated from relative polycythemia, which results from hemoconcentration due to diarrhea/ vomiting. Polycythemia vera, in contrast to reactive polycythemia, is associated with low levels of serum erythropoietin (EPO).
Genetics
Most cases (95%) are associated with JAK2 V617F mutation or JAK2 axon 12 mutation on the short arm of the 9th chromosome.
JAK2 617F mutation is also seen in nearly 50% of cases of –
- Essential thrombocythemia (ET)
- Primary myelofibrosis (PMF)
Pathogenesis
JAK2 V617F point mutation or JAK2 axon 12 mutation on the short arm of the 9th chromosome → constitutive activation on JAK2/STAT signaling pathway → sharply lowers the dependence of hematopoietic cells on growth factors for growth and survival → Dysregulated activation of JAK-STAT signaling pathway → Proliferation and differentiation of Hematopoietic progenitor cells → Too much increase in RBC, Granulocytes, and Platelets (panmyelosis) → most clinical signs and symptoms are related to an absolute increase in red cell mass → Polycythemia Vera (Primary polycythemia)
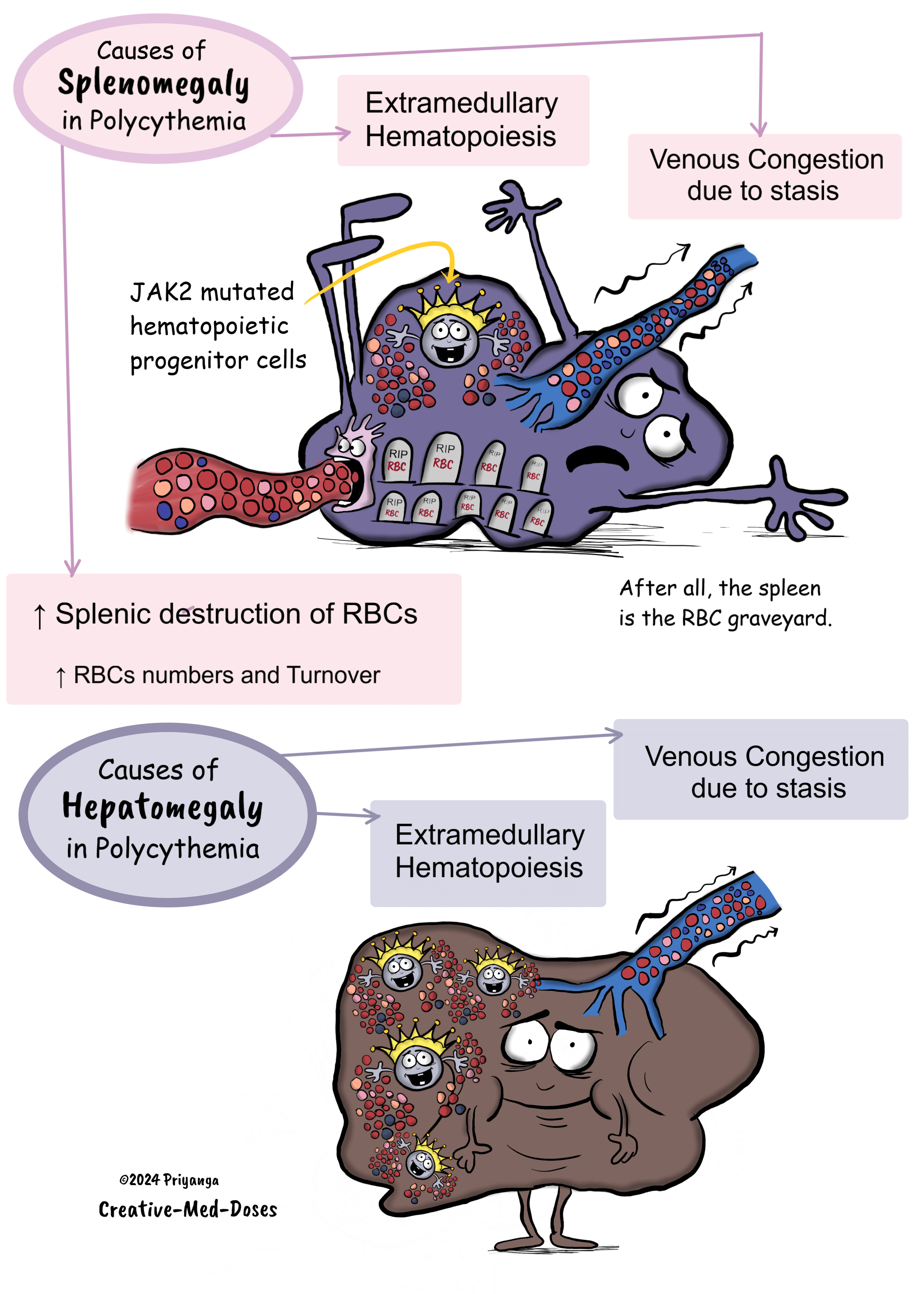
The neoplastic hematopoietic progenitor cells are also involved in extramedullary hematopoiesis in the spleen and liver resulting in hepatosplenomegaly.
Polycythemia vera, like all myeloproliferative neoplasms, can transform into a Spent phase (primary myelofibrosis) or Blast crisis (acute myeloid leukemia). Both spent phase/ blast crisis is triggered by added acquired somatic mutations.
Polycythemia vera (primary polycythemia) vs Reactive Polycythemia (secondary polycythemia)
Normal Hematopoietic progenitor cells
Ligand (EPO/TPO) dependent JAK2-STAT activation
Erythropoietin attaches to EPO receptors on Hematopoietic progenitor cells → Activation of JAK-STAT signaling pathway → Proliferation and differentiation of Hematopoietic progenitor cells → Increase in RBC, Granulocytes, and Platelets.
Hematopoietic progenitor cells with Mutated JAK2 V617F
Ligand (EPO/TPO) independent JAK2-STAT activation
Constitutive activation of JAK2-STAT signaling pathway→ Dysregulated activation of JAK-STAT signaling pathway → Proliferation and differentiation of Hematopoietic progenitor cells → Too much increase in RBC, Granulocytes, and Platelets → Polycythemia Vera (Primary polycythemia)
Hematopoietic progenitor cells in reactive erythrocytosis
Increased EPO release → Erythropoietin attaches to EPO receptors on Hematopoietic progenitor cells → activation of JAK-STAT signaling pathway → Activation of gene for growth and proliferation → Proliferation and differentiation of Hematopoietic progenitor cells → Too much Increase in RBC (Reactive erythrocytosis), Granulocytes and Platelets → Reactive (Secondary) Polycythemia
....
....
Clinical features
Increased RBCs lead to an increase in blood viscosity that is associated with
- Abnormal cerebral blood flow leading to headache
- Abnormal Retinal flow →Visual disturbance
- Increased risk of thromboembolic events
- stroke
- gangrene
- myocardial infarction
- pulmonary embolism
- deep vein thrombosis
- Microvessel thrombosis (episodic blood clots) leads to Erythromelalgia (hyperemic and painful extremities)
Dysfunctional platelets →Increased risk of thromboembolic events and bleeding
Increased number of RBCs → Increased splenic destruction of RBCs leading to → Splenomegaly
Increased RBC destruction →increased uric acid and LDH release due to cell lysis → increased uric acid levels cause the formation of uric acid crystals in Joints → Gout.
Bleeding tendencies lead to bleeding gums, epistaxis, Gastrointestinal bleeding, and ecchymoses.
Extramedullary hematopoiesis leads to hepatomegaly and splenomegaly.
Histamine released from Basophils leads to
- Pruritis (aquagenic pruritis) – itching after a hot shower.
- Peptic ulcer
Polycythemia cases can transform into a Spent phase or Blast crisis
Spent phase – Extensive fibrosis in the bone marrow. It resembles Primary myelofibrosis. Associated with Dry tap in bone marrow procedure. The hematopoiesis shifts to the spleen and liver, causing splenomegaly and hepatomegaly.
Blast Crisis- Presence of excessive blasts like AML.
.....
.....
Diagnosis
The 2016 WHO revised diagnostic criteria for Polycythemia Vera
The diagnosis of PV requires meeting either all three major criteria or the first two major criteria and minor criteria.
Major criteria
Criteria number 1 (clinical)
- Hemoglobin >16.5 g/dL in Men, >16 g/L in women, or
- Hematocrit >49% in men, >48% in women, or
- Red cell mass 25% increase above mean normal predicted value.
Criteria number 2 (morphological)*
Bone marrow morphology* Hypercellularity for age with trilineage growth (panmyelosis), including prominent erythroid, erythroid, granulocytic, megakaryocytic proliferation with pleomorphic mature megakaryocytes.
Criteria number 3 (Genetic)
Presence of JAK2 V617F mutation or JAK2 axon 12 mutation
Minor criteria
Serum erythropoietin (EPO) levels – Subnormal EPO levels
Important point*
*Bone marrow criteria may not be required in cases with sustained absolute erythrocytosis: Hb levels >18.5 g/dL in Men (hematocrit 55.5%) or >16.5 g/dL in women (hematocrit 49.5%), if major criteria number 3 and minor criteria are present.
Treatment
Phlebotomy - Elevated red cell mass blood is an important risk factor for thrombosis. Periodic phlebotomy is recommended to reduce red cell mass and prevent thrombosis incidences.
Maintain the hemoglobin level at ≤140 g/L (14 g/dL; hematocrit <45%) in men and ≤120 g/L (12 g/dL; hematocrit <42%) in women to reduce the risk of thrombotic complications.
Low-dose Aspirin to reduce the risk of thrombosis. Reduce the RBC mass by phlebotomies before using Aspirin.
Anticoagulants – to treat thrombosis.
Allopurinol for Gout.
Anagrelide- is a phosphodiesterase inhibitor that reduces the platelet count.
Cytoreductive therapy (recommended for resistant cases)
- Hydroxyurea – causes myelosuppression and reduces cell production.
- Interferon alpha (IFN-α) – reduces cell proliferation.
- Ruxolitinib- JAK inhibitor – reduces cell proliferation.
Revision for today Renal Hypoxia: Why kidney is prone to hypoxia and ischemic injury? - Creative Med Doses
Buy fun review books here (these are Kindle eBooks you can download Kindle on any digital device and log in with an Amazon account to read them). Have fun and please leave a review.