Metabolic Acidosis in Chronic Kidney Disease
Metabolic Acidosis is a condition where the body’s acid load is so high that it starts to affect the normal functioning of the body. It is defined as serum bicarbonate levels < 22 mEq/L (or serum tCO2 levels < 22 mEq/L). The lungs and kidneys play a major role in acid-base maintenance.
Serum bicarbonate and serum tCO2
Serum bicarbonate travels through the body in the form of carbon dioxide gas. High serum bicarbonate gives high levels of serum total carbon dioxide (tCO2), and low serum bicarbonate levels give low levels of serum tCO2. That’s why the serum tCO2 is a surrogate assessment marker for serum bicarbonate levels.
Normal kidney removes excess acid load by excreting more ammonia and titratable acids. In chronic kidney disease, the kidney cannot excrete excess acid due to a reduced number of functioning nephrons. It leads to the accumulation of acid in the blood and metabolic acidosis.
Metabolic acidosis and serum bicarbonate levels
The body has a carbonic acid-bicarbonate buffer system. It helps in maintaining the pH balance. The lungs and kidneys play a crucial role in regulating the acid-base balance using this buffer system.
(HCO3-) + (H+) ⇔ H2CO3 ⇔ H2O + CO2
In metabolic acidosis, where blood pH is too low, the excess hydrogen ion (H+) combines with bicarbonate ion (HCO3-)and forms carbonic acid (H2CO3). The H2CO3 later breaks down into H2O and CO2. The CO2 is removed by the lungs. That is why an increased respiratory rate is associated with metabolic acidosis. It also explains reduced serum bicarbonate levels (serum tCO2) in metabolic acidosis. Serum bicarbonate (HCO3-) is low because it gets consumed by a buffer system to neutralize the acidic hydrogen ion (H+).
Kidneys maintain the normal blood pH in cases with excess acid load in two ways-
- Increasing the bicarbonate reabsorption
- Increased excretion of Hydrogen ion (H+) in urine in the form of ammonia (NH4+) and titratable acids (H2PO4-).
Metabolic acidosis in CKD
In chronic kidney disease, there is a significant reduction in functioning nephron numbers, critically impairing the ability to excrete excess H+ ions and to reabsorb enough HCO3-, resulting in metabolic acidosis associated with CKD.
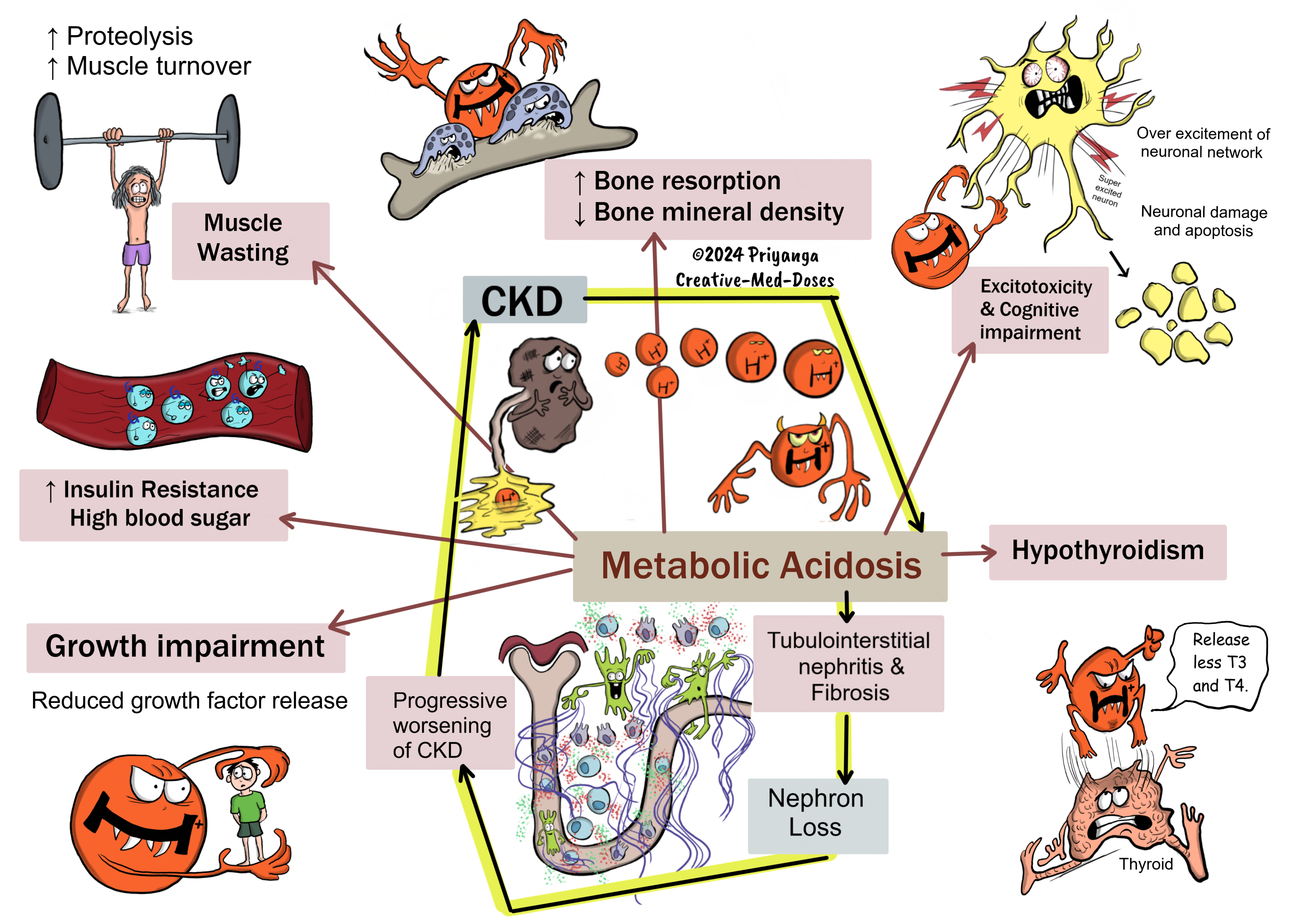
Complications
Untreated metabolic acidosis in CKD cases has the following consequences-
- Progression of CKD
- Muscle wasting
- Decreased insulin sensitivity
- Reduced bone mineral density
- Hypothyroidism
- Cognitive impairment
- Growth impairment
- Progression of CKD
Untreated acidosis leads to H+ stress in the body.
The H+ stress stimulates the production of the following –
Increased angiotensin II simulates inflammatory response in a tubulointerstitial compartment that may lead to tubulointerstitial nephritis, fibrosis, and tubular atrophy.
Endothelin-1 and Aldosterone increase tubulointerstitial inflammation and fibrosis that lead to tubular atrophy.
Increased Ammonia production
Acidosis stimulates increased ammonia production in kidneys that subsequently cause activation of the complement pathway. It increases tubulointerstitial inflammation and fibrosis.
Tubulointerstitial fibrosis and atrophy result in further reduction in functional nephron numbers and accelerate the progression of chronic kidney disease.
- Muscle wasting
Metabolic acidosis increases inflammatory cytokines and reduces muscle pH. It leads to proteolysis and increased muscle turnout rate. Metabolic acidosis also stimulates muscle atrophy. Muscle degradation and muscle wasting lead to a significant loss in muscle mass in CKD with metabolic acidosis.
- Decreased insulin sensitivity
Acidosis decreases the insulin binding to its receptors and impairs insulin-induced intracellular signaling. It results in insulin insensitivity (insulin resistance) and high blood sugar levels.
Insulin binds with insulin receptors and opens the channel for glucose entry in the cell. Insulin is the key to glucose entry in most cells in the body.
Metabolic acidosis inhibits insulin binding to the receptor, and without insulin and insulin receptor interaction, glucose cannot enter the cells. In short, metabolic acidosis blocks the glucose entry in cells. It causes increased insulin resistance or insulin insensitivity. It leads to high blood sugar levels.
- Reduced bone mineral density
It is associated with reduced pH in the blood causes low pH in the interstitial area of bone, activation of osteoclasts, and cell-mediated bone resorption. The excessive bone resorption and mineral dissolution significantly reduce bone mineral density, resulting in osteoporosis, Osteomalacia, and osteitis fibrosa cystica in patients with CKD.
- Hypothyroidism
Acidosis in CKD is associated with reduced plasma T3 and T4 levels with normal TSH levels.
- Cognitive impairment
Metabolic acidosis causes over-excitation of neural networks, leading to excitotoxicity and cognitive impairment.
- Growth impairment
Metabolic acidosis causes growth impairment in children with CKD by inhibiting the release of growth hormones.
...
....
....
Management of metabolic acidosis in CKD
The serum tCO2 (serum bicarbonate) levels < 22 mEq/L are an indication to start treatment of metabolic acidosis. Start treatment as soon as possible because even a mild degree of metabolic acidosis can increase protein catabolism and accelerate the CKD progression.
The following are management options –
- Modified diet
- Alkali Supplementation
- Newer drug - Veverimer
1. Modified diet
- Base-producing diet – eating more fruit and vegetables is known as base-producing dies as it increases serum bicarbonate levels.
- Avoid animal proteins – animal protein increases the total acid load, and minimizing its intake means less acid, which means sick kidneys of CKD have a lesser acid load.
2. Alkali Supplementation
- Oral sodium bicarbonate (most commonly used)
- Oral sodium citrate
Main side effects of alkali therapy
Sodium retention, fluid retention, hypertension, pulmonary and peripheral edema-
Since both alkali supplements (sodium bicarbonate and sodium citrate) contain sodium, high doses of alkali can lead to sodium and water retention, resulting in fluid retention, volume overload, and hypertension. Always consider the volume status of the patient before starting alkali supplementation.
Vascular calcification and kidney calcification
Calcification -The high urinary pH due to bicarbonate supplementation predisposes patients to calcium phosphate nephrolithiasis.
Due to the possibility of the above side effects, check a few parameters before initiating the pharmacological treatment-
- Severity of metabolic acidosis
- Blood pressure
- Volume status
Metabolic acidosis associated with hyperkalemia has a risk of cardiac arrhythmia, so start alkali treatment as soon as possible.
Revision for today https://creativemeddoses.com/topics-list/environmental-enteropathy-pathogenesis/
Buy fun review books here (these are Kindle eBooks you can download Kindle on any digital device and log in with an Amazon account to read them). Have fun and please leave a review.
https://creativemeddoses.com/books/