Focal Segmental Glomerulosclerosis (FSGS)
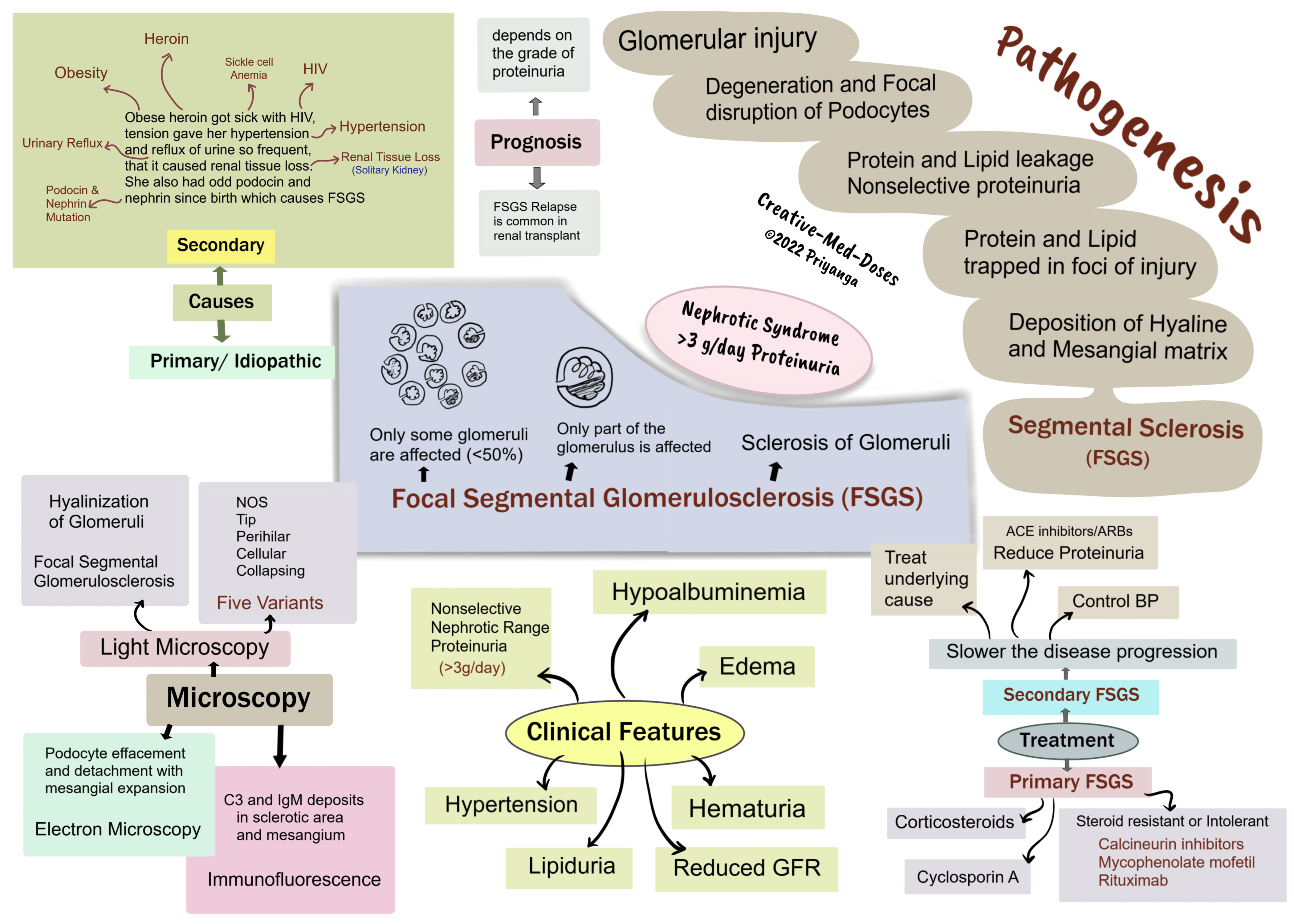
Focal segmental glomerulosclerosis (FSGS) is characterized by sclerosis of <50% of glomeruli (Focal). And sclerosis involves only a part of each affected glomerulus(segmental).
The most common Primary glomerular lesions that lead to the nephrotic syndrome are focal segmental glomerulosclerosis (in adults) and minimal-change disease (in children).
Types and causes
FSGS can be primary and secondary. This distinction has both prognostic and therapeutic implications.
Primary FSGS (idiopathic) - approximately 20% to 30% of all cases of nephrotic syndrome.
Secondary FSGS may be associated with the following conditions -
- HIV infection
- Heroin abuse
- Obesity
- Sickle cell disease
- Secondary to other forms of GN (e.g., IgA nephropathy, hypertensive nephropathy, reflux nephropathy)
- As a maladaptation to nephron loss due to chronic kidney disease or congenital malformations
- Inherited forms are associated with mutations in cytoskeletal proteins nephrin and podocin. Nephrin and podocin are essential for the integrity of podocytes.
Pathogenesis
Multiple factors/defects → Glomerular injury → Degeneration and Focal disruption of Podocytes →Decreased Glomerular barrier integrity →Protein and Lipid leakage →Nonselective proteinuria→ Nephrotic range >3g/day→ Protein and Lipid trapped in foci of injury →Deposition of Hyaline and Mesangial matrix→ Sclerosis of injured part of glomerulus →Segmental Sclerosis→ Focal Segmental Glomerulosclerosis.
Adaptive FSGS
Hypertension-related renal damage→ Loss of autoregulation of renal blood flow at the afferent arteriole
→Transmission of elevated pressures to an unprotected glomerulus →Leading to hyperfiltration and hypertrophy→ Increased fibrosis and sclerosis→ Eventual focal segmental glomerular sclerosis.
Morphology
Light microscopy- focal segmental sclerosis and hyalinization of glomeruli. Juxtamedullary nephrons are affected first, and inadequate sampling may miss focal lesions.
Histological Variants- FSGS is classified into five variants:
Not Otherwise Specified (NOS)- It is the most common variant of FSGS
Tip – the segmental lesion involves a tubular pole of the glomerulus.
Perihilar – sclerosis and hyalinization at the vascular pole of the glomerulus. It is present in cases with hyperfiltration and adaptive response where glomerular pressure is very high.
Cellular- hypercellular glomerulus with endocapillary and epithelial hyperplasia is characteristic of this variant.
Collapsing- is characterized by the collapse of the glomerular tuft and epithelial cell hyperplasia. It has the lowest rate of remission and the worst prognosis.
Immunofluorescence – C3 and IgM deposits in sclerotic area and mesangium.
Electron Microscopy –shows podocyte effacement and detachment with mesangial expansion.
Clinical presentation
FSGS and minimal change disease is associated with nephrotic syndrome, but the incidence of hematuria and hypertension is higher in individuals with FSGS. It is crucial to differentiate between FSGS and minimal change disease because treatment and clinical course vary.
FSGS associated proteinuria is nonselective, and minimal change disease has selective proteinuria.
Minimal change disease has a better steroid response. FSGS cases have poor steroid response as compared to minimal change disease cases.
FSGS can present with
- Hematuria
- Hypertension
- Nephrotic-range proteinuria (>3g/day)
- Lipiduria
- Renal insufficiency and reduced GFR
Treatment
Primary FSGS treatment -
- Corticosteroids
- Immunosuppressive therapy with calcineurin inhibitors (CNI), mycophenolate mofetil, or rituximab in patients resistant or intolerant to steroids
- Cyclosporin A
- Renal transplant in ESRD
- Plasmapheresis - Primary FSGS recurs in 25–40% of patients with renal transplants. In recurrent post-transplant FSGS cases, plasmapheresis can achieve remission.
The treatment of secondary FSGS is targeted toward slowing the disease progression and treating the underlying cause.
- Treat the underlying cause
- Controlling proteinuria- inhibitors of the renin-angiotensin system (ACE inhibitor and ARBs)
- Treat Hypertension
- No role for steroids or other immunosuppressive agents in secondary FSGS
- Statin therapy for hypercholesterolemia
- Anticoagulation in patients at risk for thrombosis or embolization
Prognosis
- Prognosis depends on the grade of proteinuria
- FSGS Relapse is common in renal transplant
...
...
Revision for today's Renal Hypoxia: Why kidney is prone to hypoxia and ischemic injury? - Creative Med Doses
Buy fun review books here (these are kindle eBook you can download kindle on any digital device and log in with Amazon accounts to read them). Have fun and please leave a review.
https://creativemeddoses.com/books/