Duchenne muscular dystrophy illustrations
Duchenne muscular dystrophy illustrations and theory for quick review 👇😋.
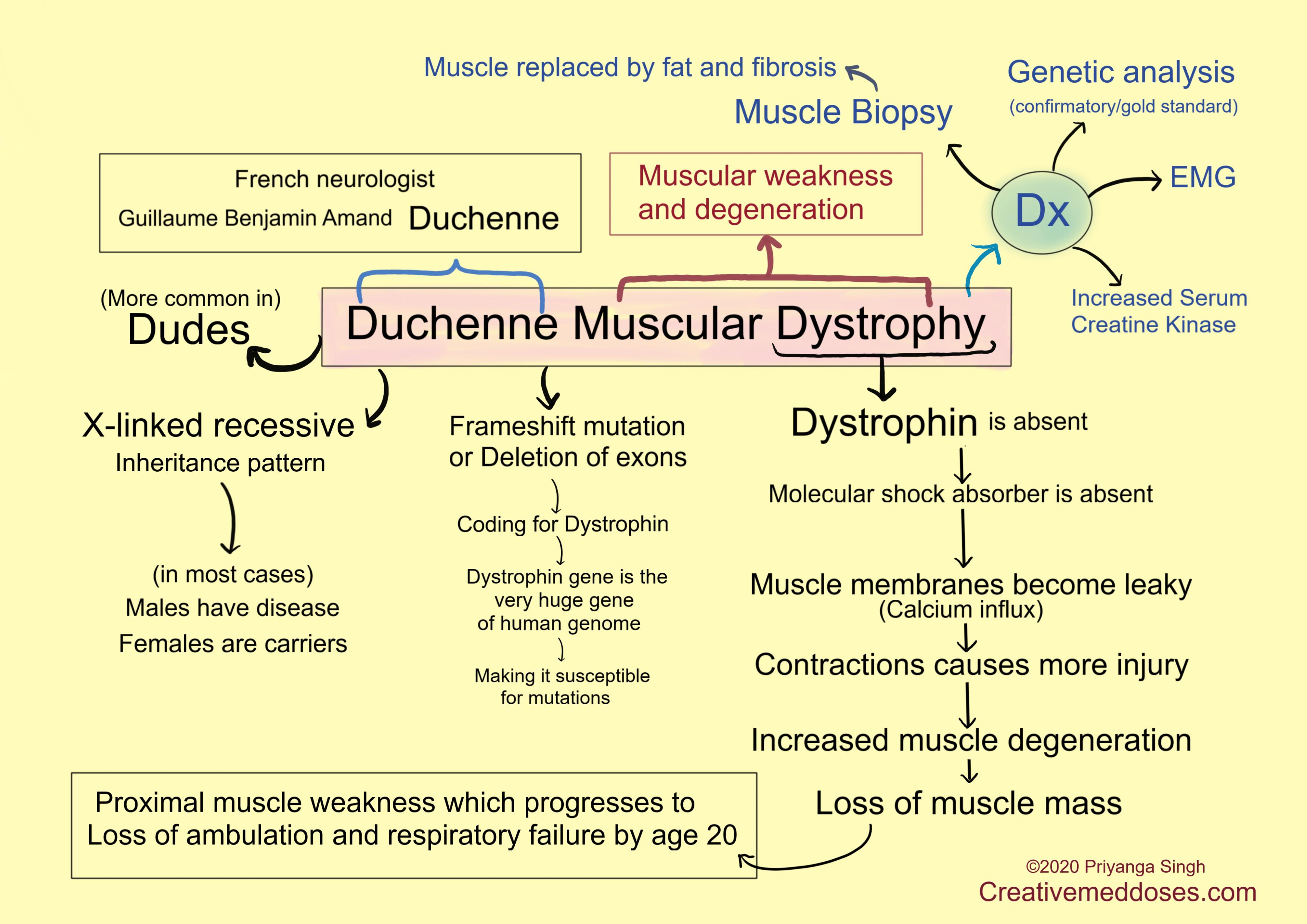
Duchenne muscular dystrophy (DMD) is X-linked recessive disease which causes lack of the cytoskeletal protein dystrophin leading to marked striated muscle degeneration. Males have only one X chromosome and this is X linked recessive disease hence it affects males more. Females typically are carriers of the genetic trait while males are affected.
It is the most common type of muscular dystrophy, affecting 1/3500 live male births.
In DMD there is frameshift mutation or deletion of the dystrophin gene which results in complete loss of dystrophin. Dystrophin is a huge gene and large size of the gene contributes to its high rate of spontaneous mutation.
What is Dystrophin?
Dystrophin is part of a large membrane-spanning complex of glycoproteins also called dystrophin glycoprotein complex (DGC). This complex is a network of proteins that physically connect the extracellular matrix to the cytoskeleton, through the muscle membrane or sarcolemma. This large multicomponent complex has both mechanical stabilizing and signaling roles in interactions between the cytoskeleton, membrane, and extracellular matrix.
Dystrophin stabilizes the muscle membrane against the forces associated with contraction acting as a “molecular shock absorber” which protects muscle membrane.
The loss of dystrophin and associated proteins at the sarcolemma leads to leaky membrane and cause contraction-induced injury. The injured muscle releases creatine kinase, it is a clinical hallmark of the disease.
Mutations in the X-linked dystrophin gene produce Duchenne muscular dystrophy (DMD), the milder Becker muscular dystrophy (BMD), and X-linked dilated cardiomyopathy (XLDCM). Cardiomyopathy is frequent in both DMD and BMD.
Clinical features – signs and symptoms
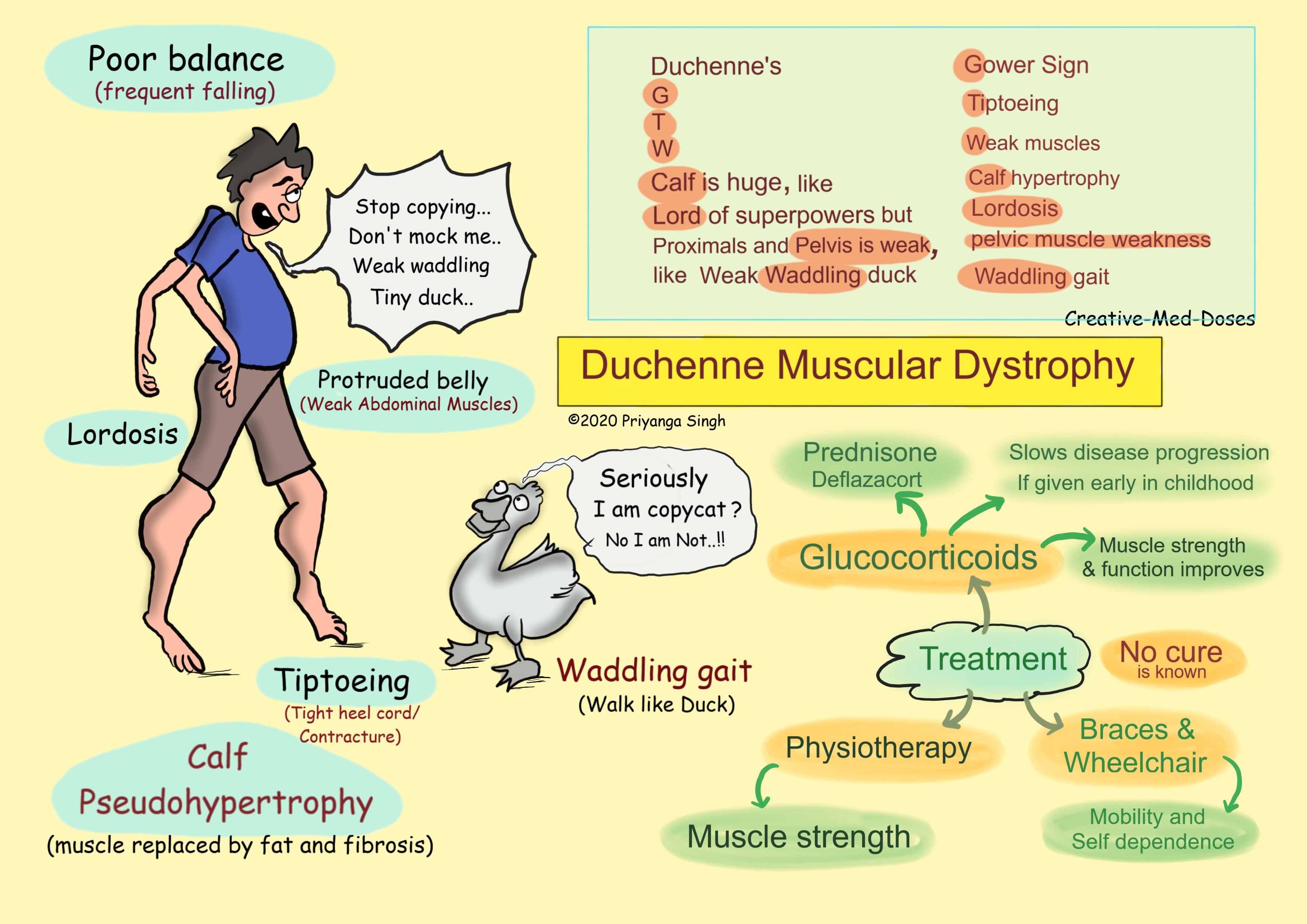
- Progressive Muscle Weakness --proximal muscles are weaker than the distal and are symmetrically affected, and the facial muscles are spared, a pattern referred to as limb-girdle weakness. Pelvic girdle muscles are especially involved earlier in disease.
- Tiptoeing
- Poor balance
- Loss of ambulation around puberty (wheelchair dependence)
- Pathologic fatigability--an inability to maintain or sustain a force
- Waddling gait- it is also called myopathic gait, the affected patient walks like a duck. Walking like a duck means that when walking the part of the pelvis of the leg moving forward moves outward and the part of the leg which is normally placed moves inward. The reason for waddling gait abnormality is weakness of the proximal muscles of the pelvic girdle which causes weakness of the gluteus muscles. Patient uses circumduction to compensate for gluteal weakness.
- Gower sign - In 1879, neurologist William Richard Gowers described the most significant Gowers sign as the characteristic patterns observed in patients with Duchenne muscular dystrophy wherein they 'climb up' their thighs with the aid of their hands to overcome the weakness of their pelvic and proximal lower limb muscles.
- Lumbar lordosis
- Calf muscle pseudohypertrophy (enlarged calves)- In Duchene muscular dystrophy (DMD), the muscles waste away and are replaced by fat and scar tissue - a process termed as fibrosis. This renders a false appearance of grossly enlarged muscles, referred to as pseudohypertrophy. The pseudohypertrophy is most prominent in the calf muscles initially, as they are overused while functioning to stabilize the body against gravity.
...
...
Diagnosis
Genetic counseling is advised for people with a family history of the disorder. DMD can be detected with about 95% accuracy by genetic studies performed during pregnancy.
Genetic analysis- gold standard and confirms the diagnosis
Muscle biopsy- muscle fibril degeneration, regeneration, and isolated fiber hypertrophy and muscle replacement with fat and connective tissue.
Serum Creatine kinase is elevated
Electrodiagnostic Studies (EMG)- repetitive nerve stimulation, and nerve conduction studies are helpful in differentiating myopathies from neuropathies and neuromuscular junction diseases.
Treatment
No cure for DMD is known
Glucocorticoids slow progression - prednisolone and deflazacort are given to improve muscle strength and function.
Physical therapy
Orthopedic appliances
Braces and Wheelchairs may improve mobility and the ability for self-care.
Form-fitting removable leg braces that hold the ankle in place during sleep can defer the onset of contractures.
...
...
Case scenario
A 5-year-old boy presents to pediatrician with proximal muscular weakness and calf muscle hypertrophy. On examination he has waddling gait and Gower’s sign is positive. His muscle strength is symmetrically reduced. Lab studies reveal increased serum creatine kinase. Muscle Biopsy from calf muscles show muscle fibril degeneration, necrosis and muscle replacement with fat and connective tissue. Which of the following drug is most likely to slower the disease progression?
A. Glucocorticoids
B. Mexiletine
C. Administration of potassium
D. Colchicine
Revision for today https://creativemeddoses.com/topics-list/osteopetrosis-cartoons-and-illustrations/
Further watching https://www.youtube.com/watch?time_continue=211&v=t3uQIS9k4_Y&feature=emb_logo