Congenital Hypertrophic pyloric stenosis (CHPS)
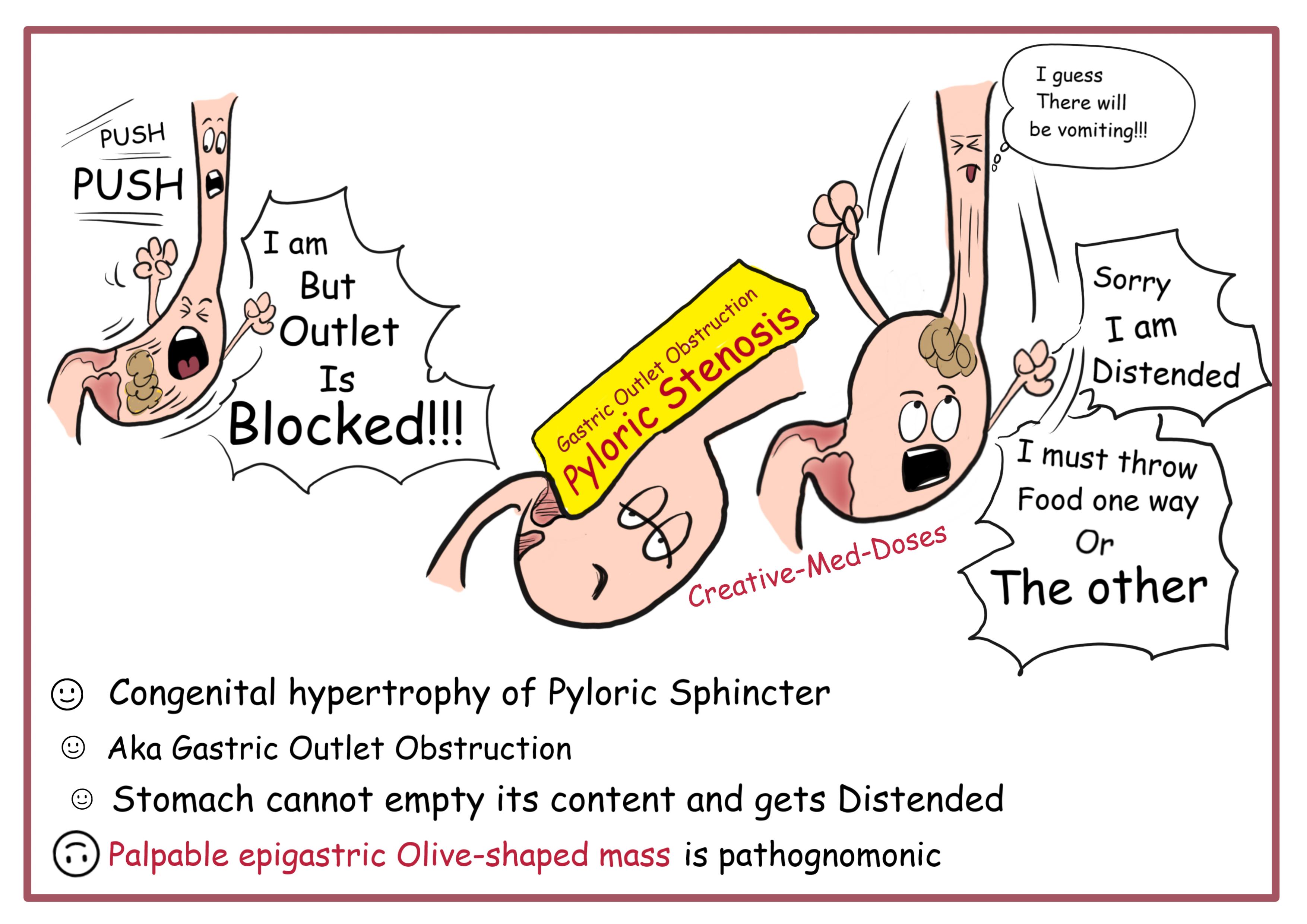
Congenital Hypertrophic pyloric stenosis (CHPS) is the idiopathic thickening of gastric pyloric musculature which later results in progressive gastric outlet obstruction.
...
...
Clinical presentation
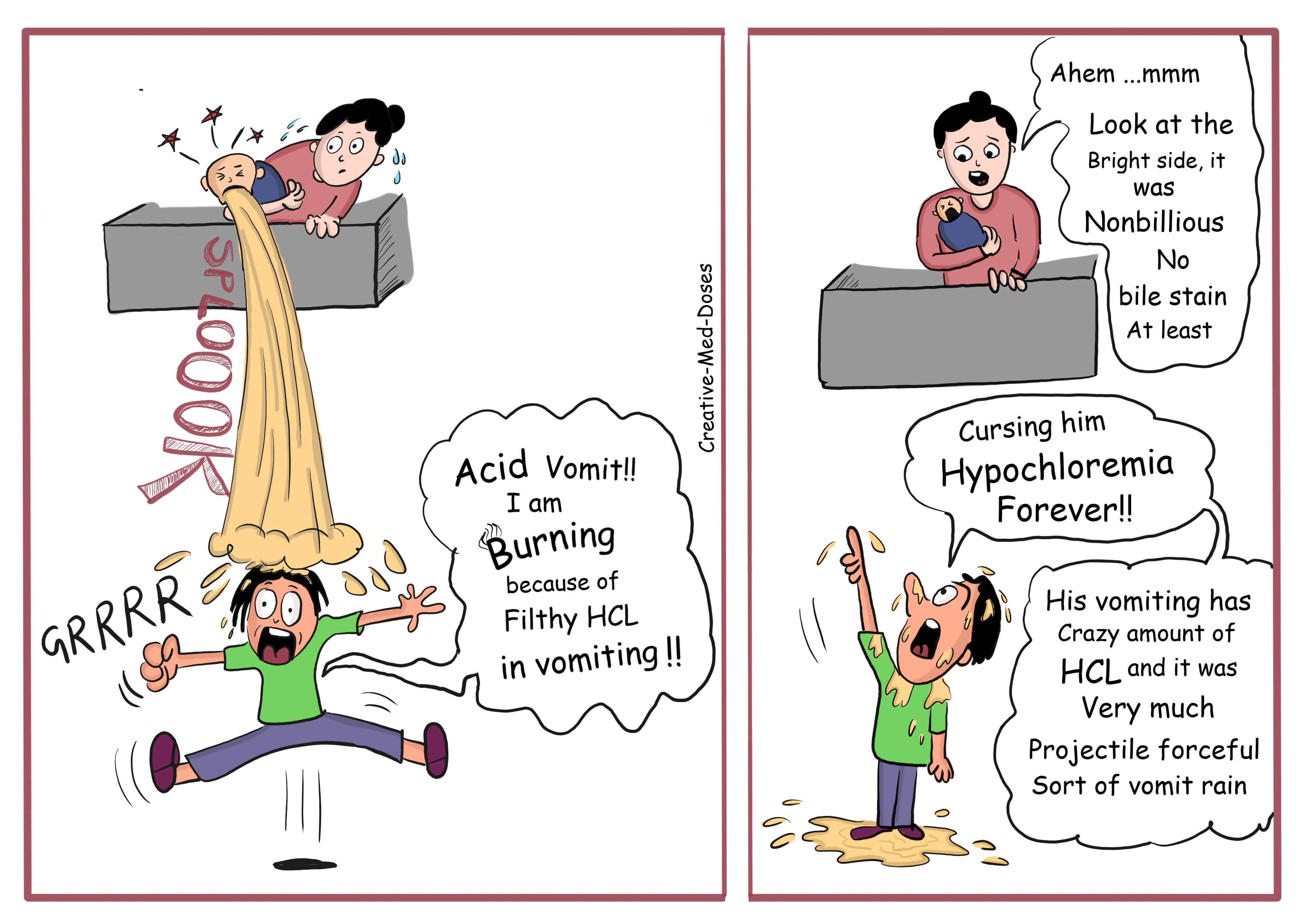
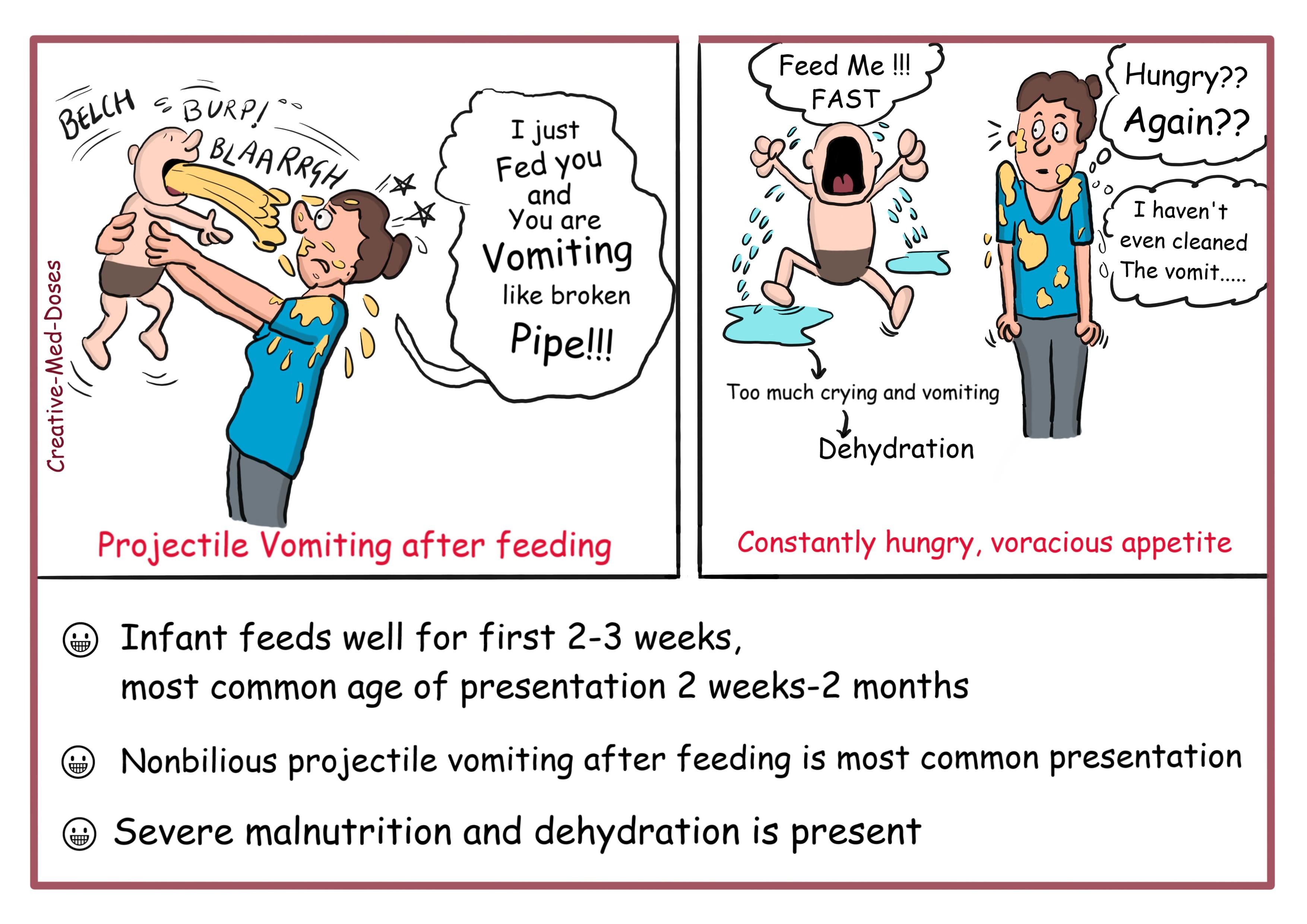
Symptoms typically clinically manifests between 6 to 12 weeks of age. The presentation is typical with non-bilious projectile vomiting. The hypertrophied pylorus is palpated as an olive-sized mass in the right upper quadrant. A succussion splash can be heard hours after the last meal. Due to the loss of hydrochloric acid in the gastric contents from persistent vomiting, there is electrolyte imbalance, specifically the characteristic hypochloremic metabolic alkalosis.
The baby in early stage of the disease remains hungry and sucks vigorously after episodes of vomiting. Delay in diagnosis can lead to dehydration, malnutrition, metabolic alterations, and lethargy. The pyloric stenosis can be associated with Turner syndrome, tracheo-esophageal fistula, esophageal atresia and trisomy 18.
...
...
Diagnosis
The diagnosis is easily made if the presenting clinical features are typical, with projectile vomiting, visible peristalsis, and a palpable pyloric tumor. An enlarged pylorus, described as an "olive," can be palpated in the right upper quadrant or epigastrium of the abdomen.
Ultrasound is the modality of choice, and Muscle wall thickness 3 mm or greater and pyloric channel length 14 mm or greater are considered abnormal in infants younger than 30 days.
Barium meal Upper GI study reveals delayed gastric emptying, peristaltic waves (caterpillar sign), elongated pylorus with a narrow lumen (string sign). The entrance to the pylorus looks like beak (beak sign)
...
...
Treatment
Initial medical management is to deal with rehydration and correction of electrolyte imbalances. This must be completed prior to surgical intervention. Definitive Treatment is surgical with a pyloromyotomy in which the pyloric muscle is divided down to the submucosa. This can be performed both open and laparoscopically.
The patient should not be operated on until there has been adequate fluid and electrolyte resuscitation. These patients need a resuscitation fluid of full-strength, balanced salt solution and, after the infant begins to urinate, the addition of potassium.
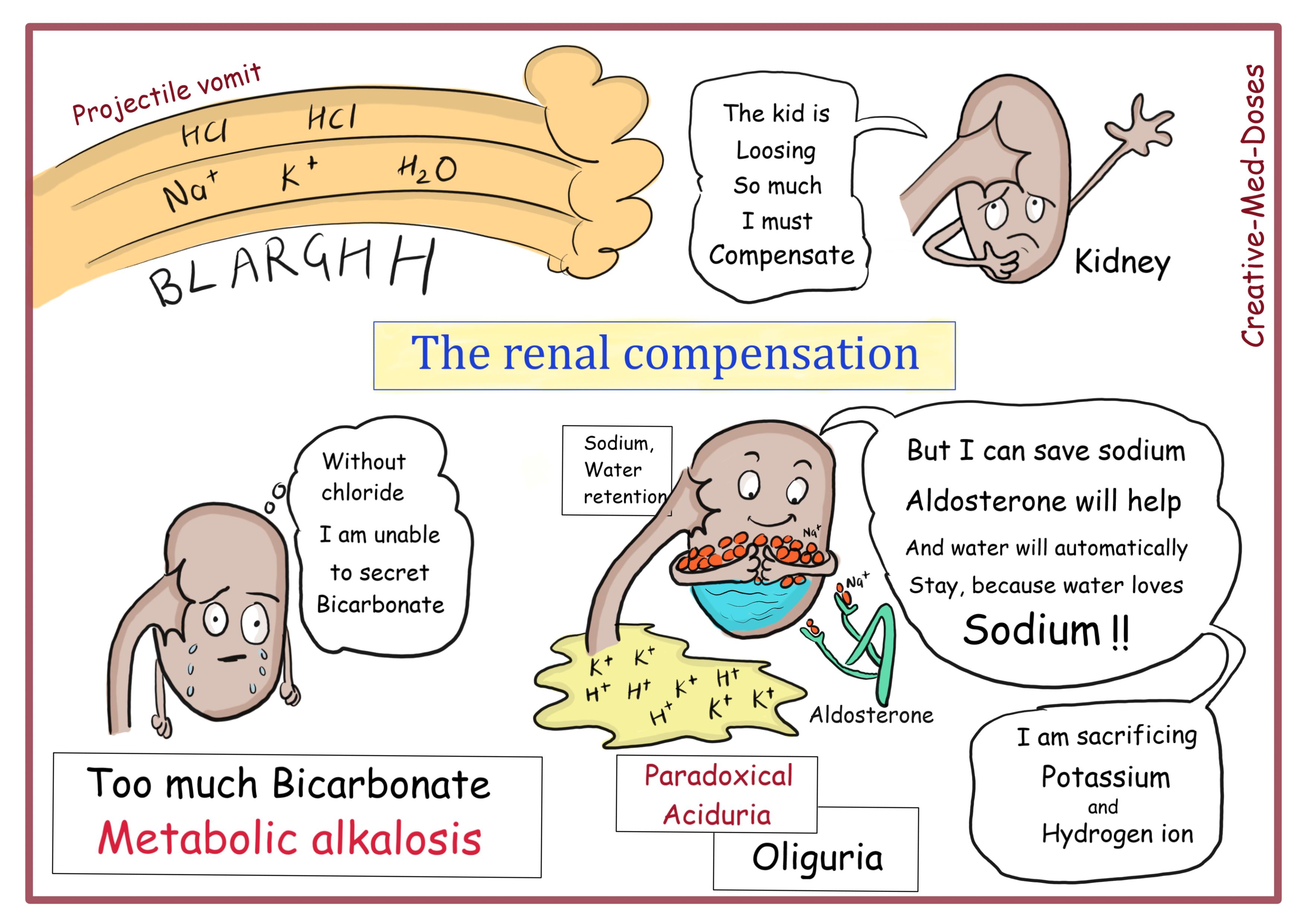
The cardinal findings in pyloric stenosis are dehydration, metabolic alkalosis, hypochloremia, and hypokalemia. Loss of gastric fluid leads to volume depletion and loss of sodium, chloride, acid (H+) and potassium. This results in a hypokalemic, hypochloremic metabolic alkalosis.
The kidneys attempt to maintain normal pH by excreting excess HCO3. But in pyloric stenosis kidney can’t excrete HCO3 because of low Chloride levels.
The kidneys attempt to conserve sodium at the expense of hydrogen ions, which can lead to paradoxical aciduria. In more severe dehydration, renal potassium losses are also accelerated owing to an attempt to retain fluid and sodium.
...
...
Case scenario: A
5-week-old boy presents to pediatrician with non-bilious projectile vomiting
which is occurring after feeding. After vomiting, the infant is
instantly hungry. The infant has dehydration and looks malnourished. On
palpation, “olive-like” mass of about 2 cm in diameter is noticed in epigastrium.
Barium studies show “Beak sign”.
Which is the most likely acid base imbalance in this infant?