Clostridium difficile
...
...
C. difficile is a spore-forming, anaerobic, Gram-positive bacillus.
Spores produced by C. difficile are heat-resistant, gastric acid and biocidal cleaning products resistant and can remain viable for months on surfaces, it can survive to hospital cleaners and even solutions that are used to disinfect the hands by healthcare professionals.
The ability to produce spores is of most important in the transmission of C. difficile, leading to frequent recurrences after successful initial treatment.
C. difficile is the leading cause of nosocomial diarrhea in hospital setup, and it is directly related to the length of hospital stay.
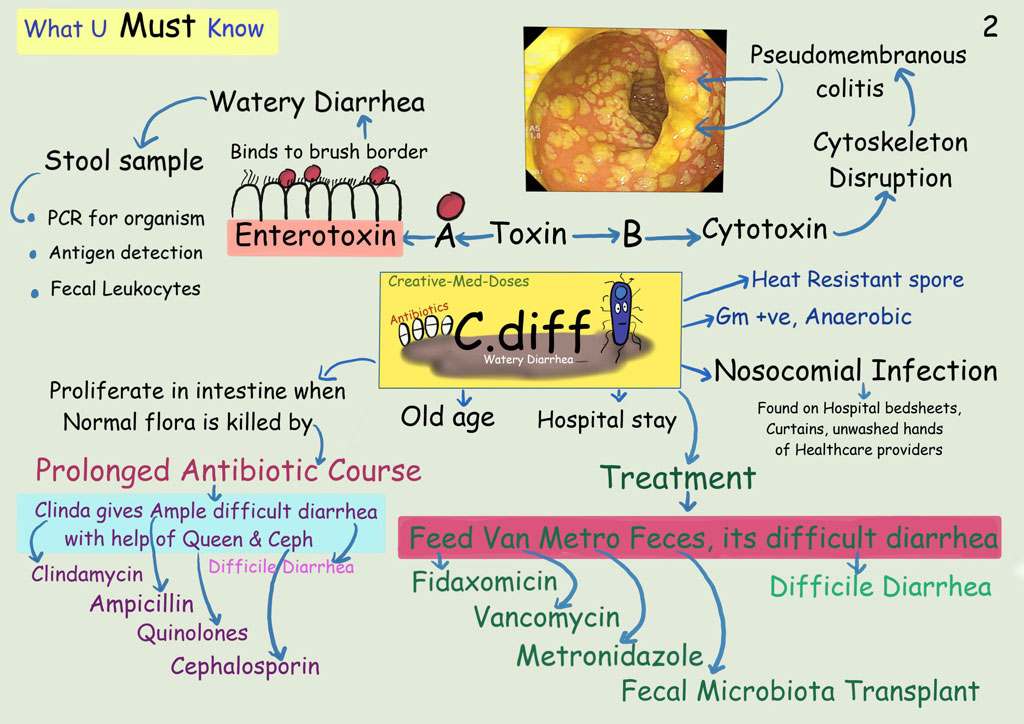
The major risk factor for C. difficile associated watery diarrhea is exposure to antibacterial therapy, classically broad-spectrum agents, clindamycin, ampicillin, cephalosporins, or fluoroquinolones. These antibiotics are disrupting colonic microflora, and favor C. difficile proliferation.
Older age (≥ 65 years old), previous hospitalization, severity of underlying disease, immunocompromised state, suppression of gastric acid secretion, tube feeding, and gastrointestinal surgery, chemotherapy and obesity are other risk factors.
The clinical presentation due to colonization and infection by C. difficile range from asymptomatic carrier to mild to moderate watery diarrhea or Pseudomembranous colitis.
Pseudomembranous colitis is one of the most serious manifestations with high mortality. The clinical presentation is caused by toxins A and B, produced by C. difficile, responsible for inflammation, damage the lining of the colon and cause inflammation leading to diarrhea and colitis, toxin A is an enterotoxin that binds to the intestinal brush border, toxin B is a cytotoxin and depolymerizes actin, disrupting the cytoskeleton.
It causes a pseudomembranous colitis and diarrhea characterized by yellow-white plaques in intestinal mucosa. Patient presents with crampy abdominal pain, abdominal tenderness and watery diarrhea.
Treatment:
Fidaxomicin, Vancomycin, Metronidazole and fecal microbiota transplant.
Complications: Toxic Megacolon