Budd-Chiari Syndrome (BCS)
Budd-Chiari Syndrome (BCS) is a rare condition associated with obstruction of two or more major hepatic veins leading to hepatic venous outflow obstruction.
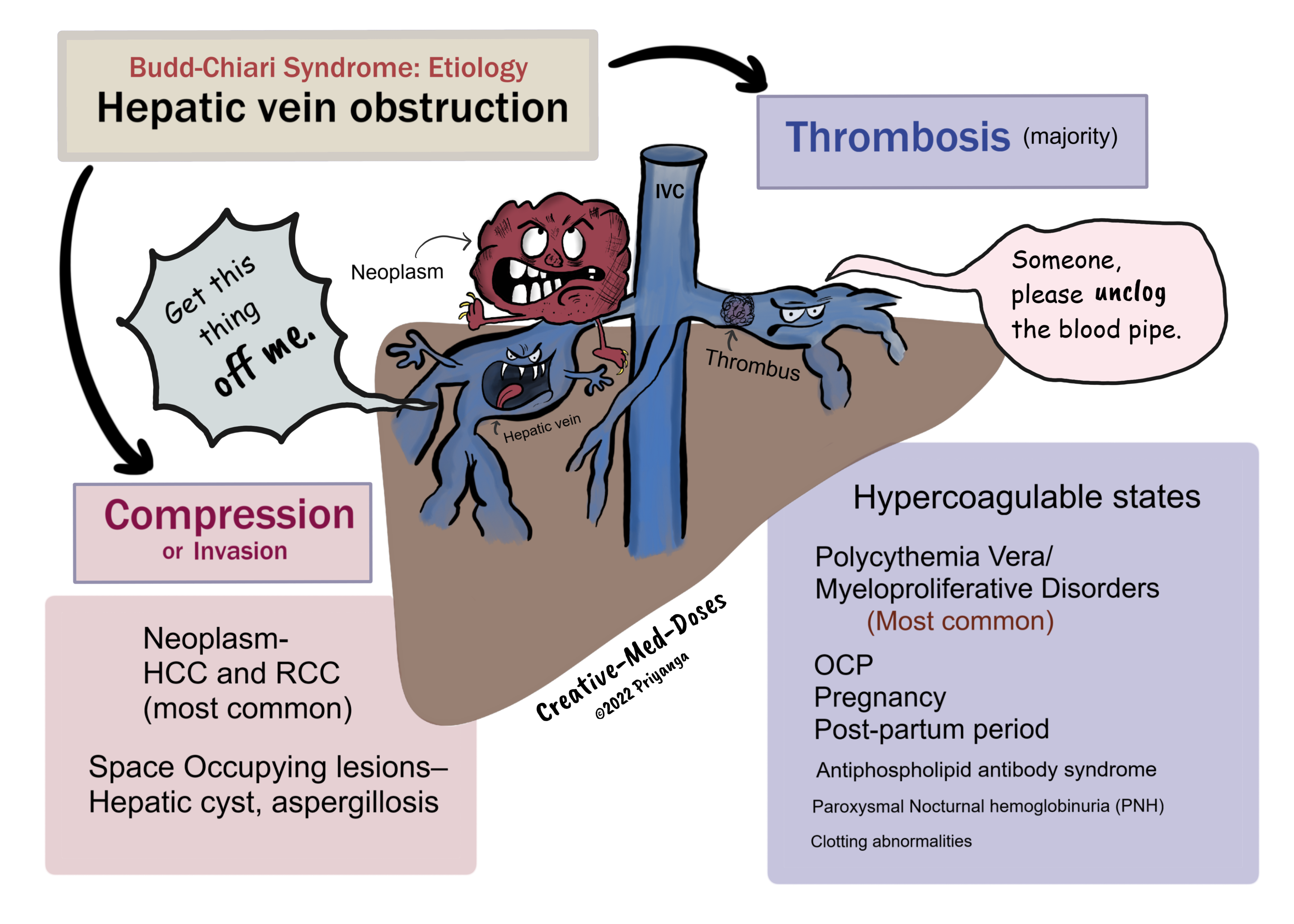
Etiology
Hepatic Venous Outflow obstruction in Budd-Chiari Syndrome can be due to-
- Thrombosis of Hepatic veins
- Compression / Invasion of Hepatic veins
Thrombosis of Hepatic veins
Most cases are associated with hypercoagulable states causing thrombosis in hepatic veins. The most important causes are the following-
- Polycythemia Vera/ Myeloproliferative Disorders – nearly 50% of cases with Budd-Chiari Syndrome are associated with myeloproliferative disorders (Polycythemia vera is most common).
- OCP/ Pregnancy / Post-partum period – all are hypercoagulable states
- Antiphospholipid antibody syndrome
- Paroxysmal Nocturnal hemoglobinuria (PNH)
- Clotting abnormalities
Compression/Invasion of the Hepatic Vein
- Neoplasm- Intrabdominal malignancies (HCC and RCC are most common)
- Space Occupying lesions Liver – Hepatic cyst, aspergillosis
...
....
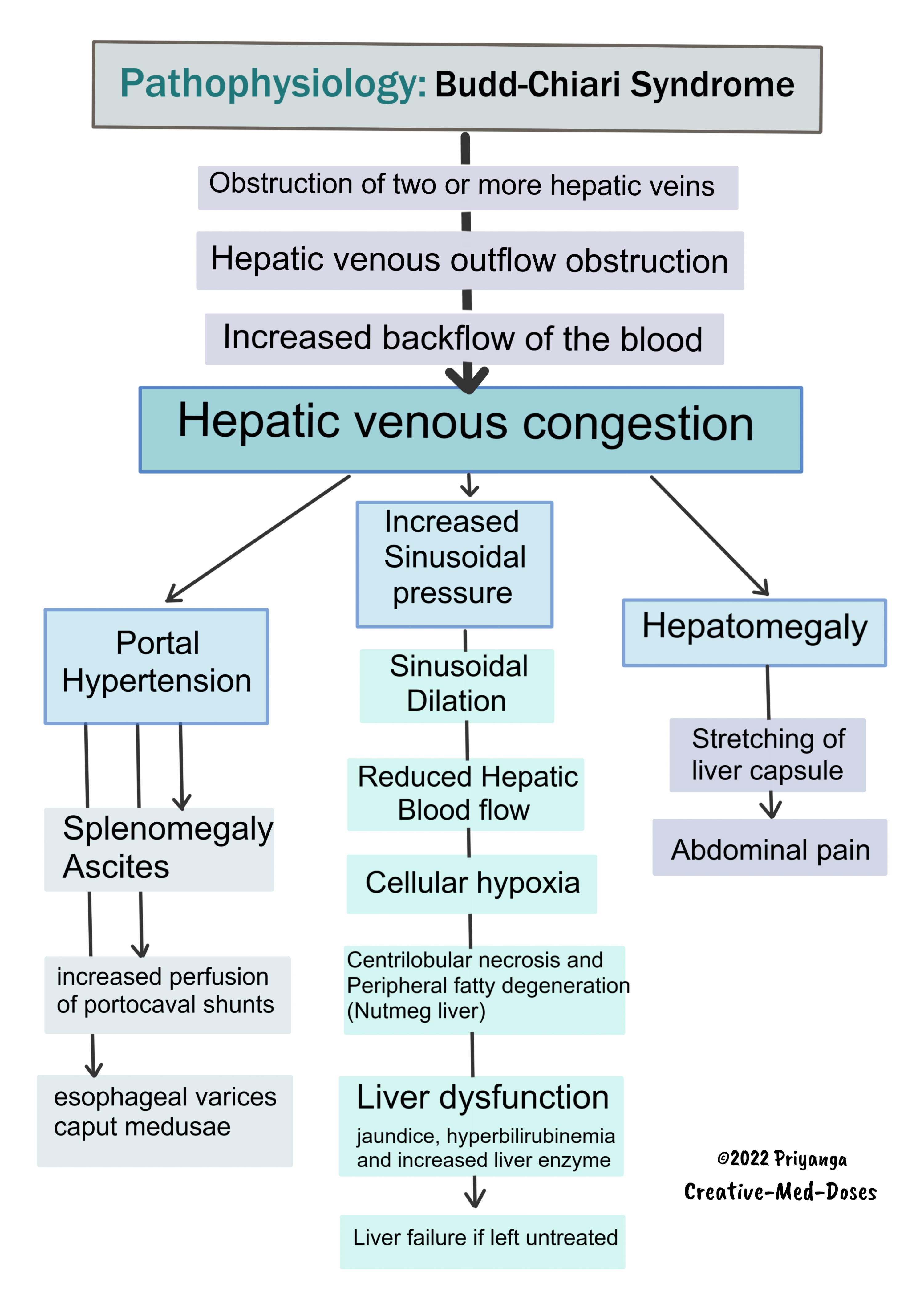
Pathophysiology
Obstruction of two or more hepatic veins →hepatic venous outflow obstruction→ impaired blood drainage to inferior vena cava→ increased backflow of the blood →hepatic venous congestion
Hepatic venous congestion→ hepatomegaly →stretching of liver capsule →abdominal pain and tender hepatomegaly
Hepatic venous congestion→ increases sinusoidal pressure → sinusoidal dilation →reduced hepatic blood flow→ cellular hypoxia→ centrilobular necrosis and peripheral fatty degeneration (Nutmeg liver) →liver dysfunction →jaundice, hyperbilirubinemia and increased liver enzyme→ liver failure if left untreated
..
..
Hepatic venous congestion may cause portal hypertension that can lead to
- splenomegaly
- ascites
- increased perfusion of portocaval shunts causing esophageal varices and caput medusae
Histopathology
- Centrilobular necrosis and peripheral fatty degeneration give the liver a “Nutmeg appearance”
- Sinusoidal dilation
- Macro nodules can be seen
Clinical features
- Abdominal pain, tender hepatomegaly (due to stretching of liver capsule), and ascites (the triad of Budd-Chiari Syndrome)
- Splenomegaly
- Jaundice
- Esophageal varices
- Caput Medusae
BCS has three categories based on disease duration and severity
- acute
- subacute
- chronic
Acute BCS has rapid disease progression (a few weeks), and the patient presents with intractable ascites and hepatic necrosis.
Subacute BCS has insidious disease progression (>3 months), and the patient often presents with hepatic necrosis but minimal ascites (development of venous collaterals).
Chronic BCS has slower progression, and the patient presents with liver cirrhosis and venous collaterals.
Diagnosis
- Clinical presentation and history
- Doppler Ultrasonography (initial investigation) – to visualize thrombosis or hepatic vein obstruction.
- CT/MRI – Confirmatory test (non-invasive modality of choice)
- Venography- gold standard test, reserved for cases with a high level of suspicion where other modalities have failed
Treatment
- Treat underlying cause
- Prevent propagation of the thrombus – use anticoagulants
- Restore blood flow by localized thrombolysis or angioplasty and Stenting
- TIPS (Trans jugular intrahepatic portosystemic shunt)
- Liver transplant in case of hepatic failure
Read more books here Books - Creative Med Doses
Revision for today Urinary Tract Infection: Treatment - Creative Med Doses