Amniotic Fluid Embolism
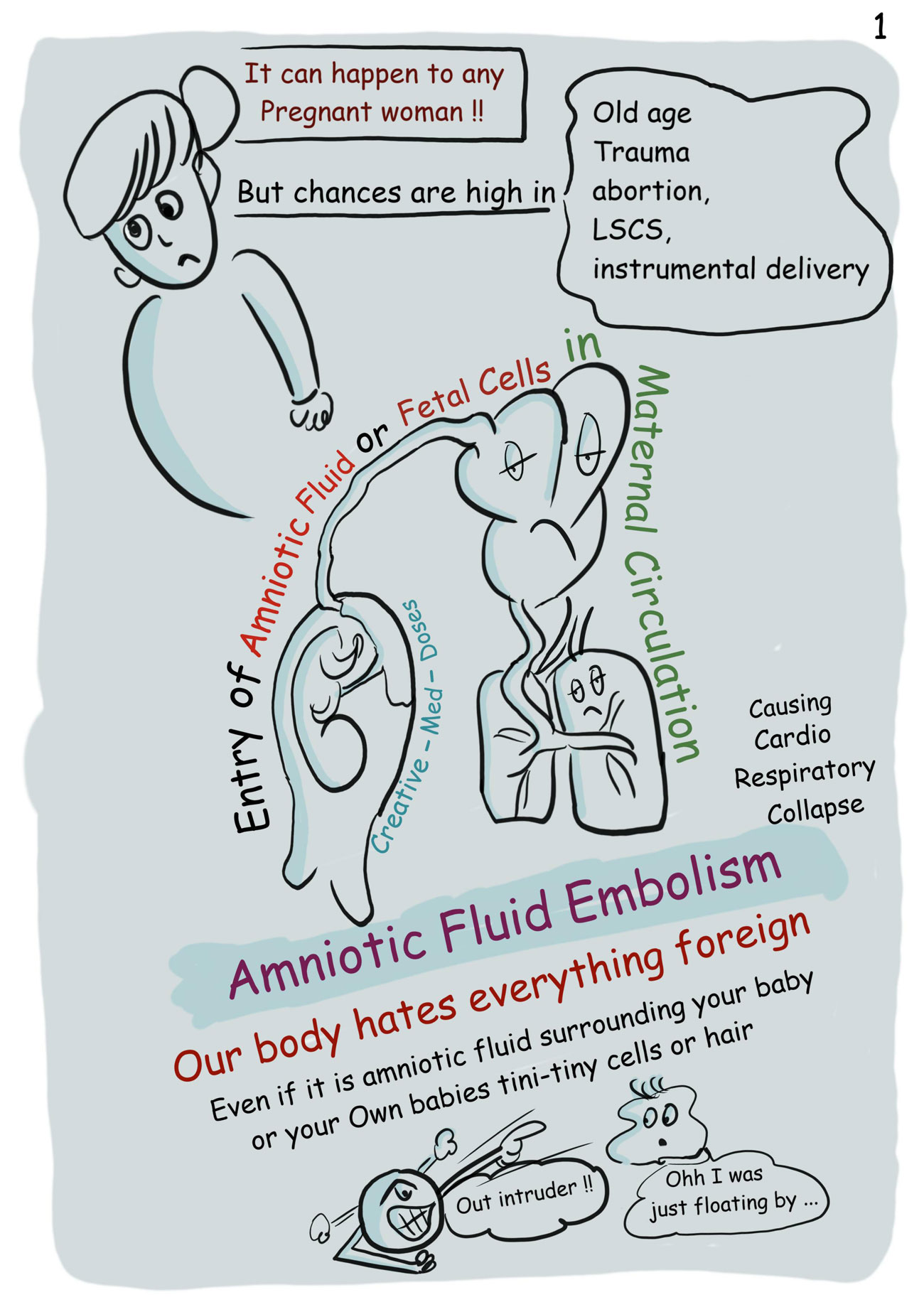
Amniotic fluid embolism (AFE) is one of the catastrophic complications of pregnancy.
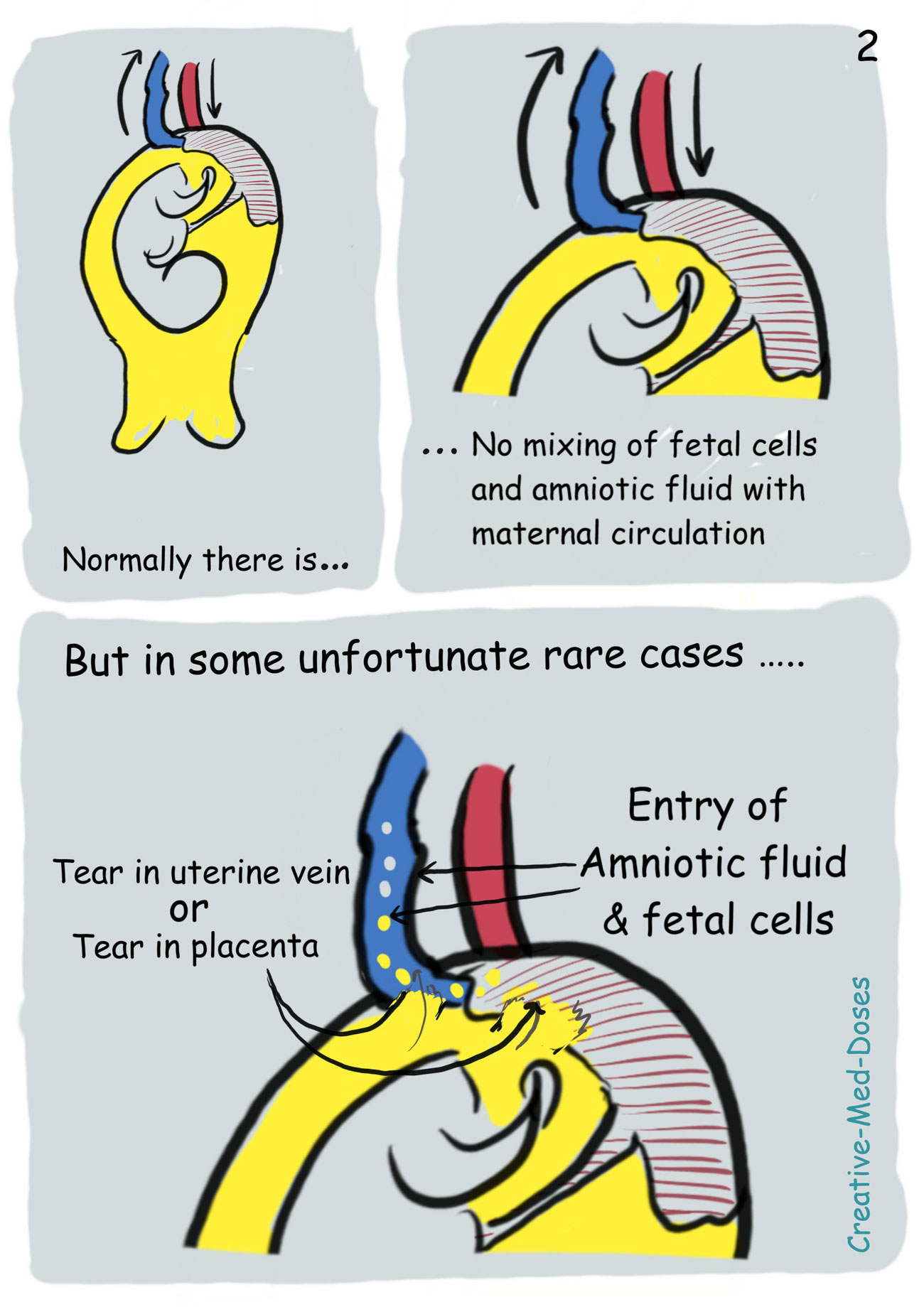
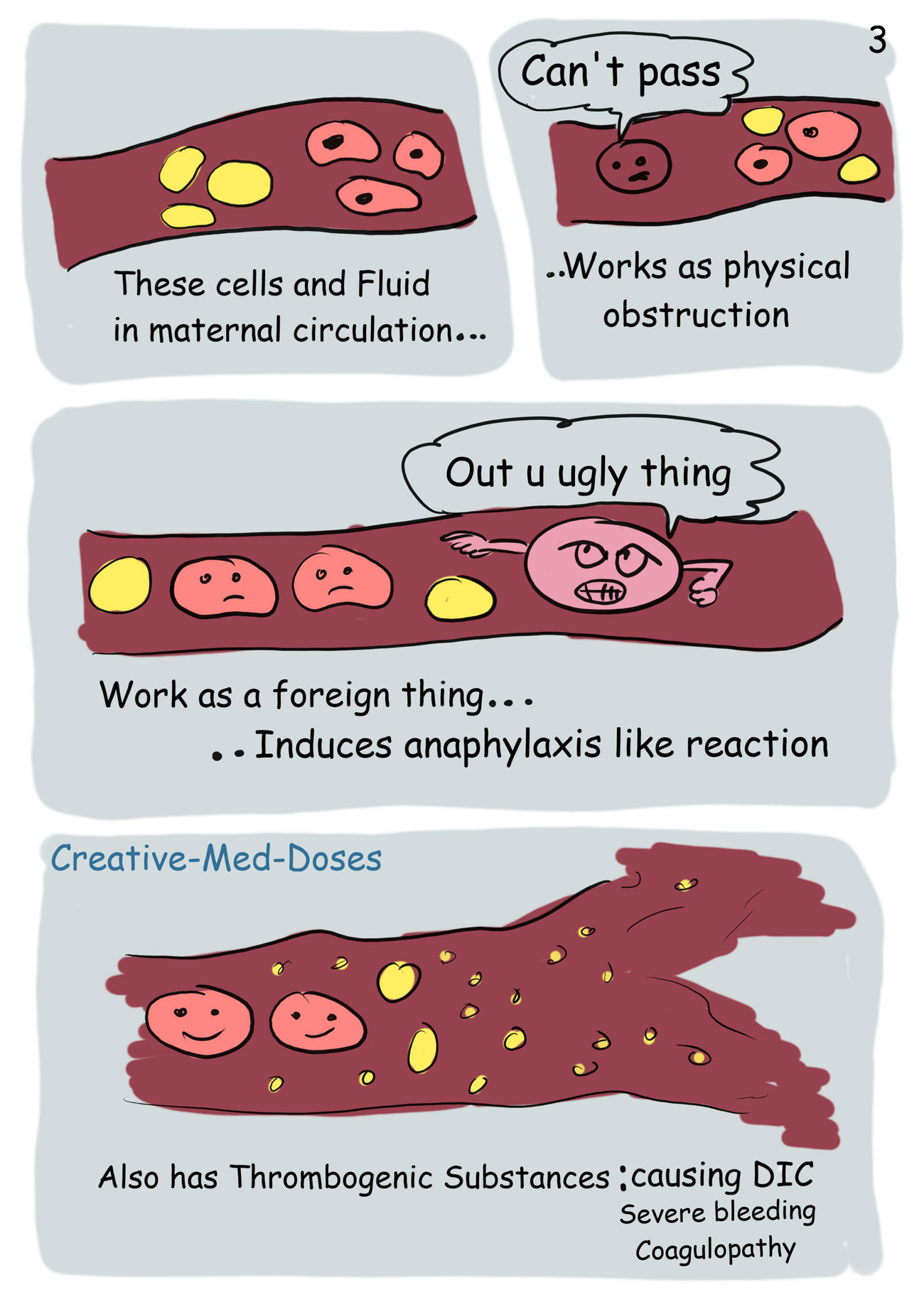
Amniotic fluid, fetal cells, hair, or other debris enters the maternal pulmonary circulation, leading to cardiovascular collapse.
Etiology is unknown, it may occur in healthy women during labour, during cesarean section, after abnormal vaginal delivery, or during the second trimester of pregnancy. It can also occur up to 48 hours post-delivery.
Clinical signs and symptoms are acute dyspnea, cough, hypotension, cyanosis, fetal bradycardia, encephalopathy, acute pulmonary hypertension, and coagulopathy.
AFE is a consequence of a humoral effect causing anaphylactoid reactions or complement activation. It is also called as “anaphylactoid syndrome of pregnancy”.
The cause of AFE-associated reactions is explained by two hypotheses:
- The effect of amniotic fluid itself
- host idiosyncrasy ("hypersensitivity" reaction)
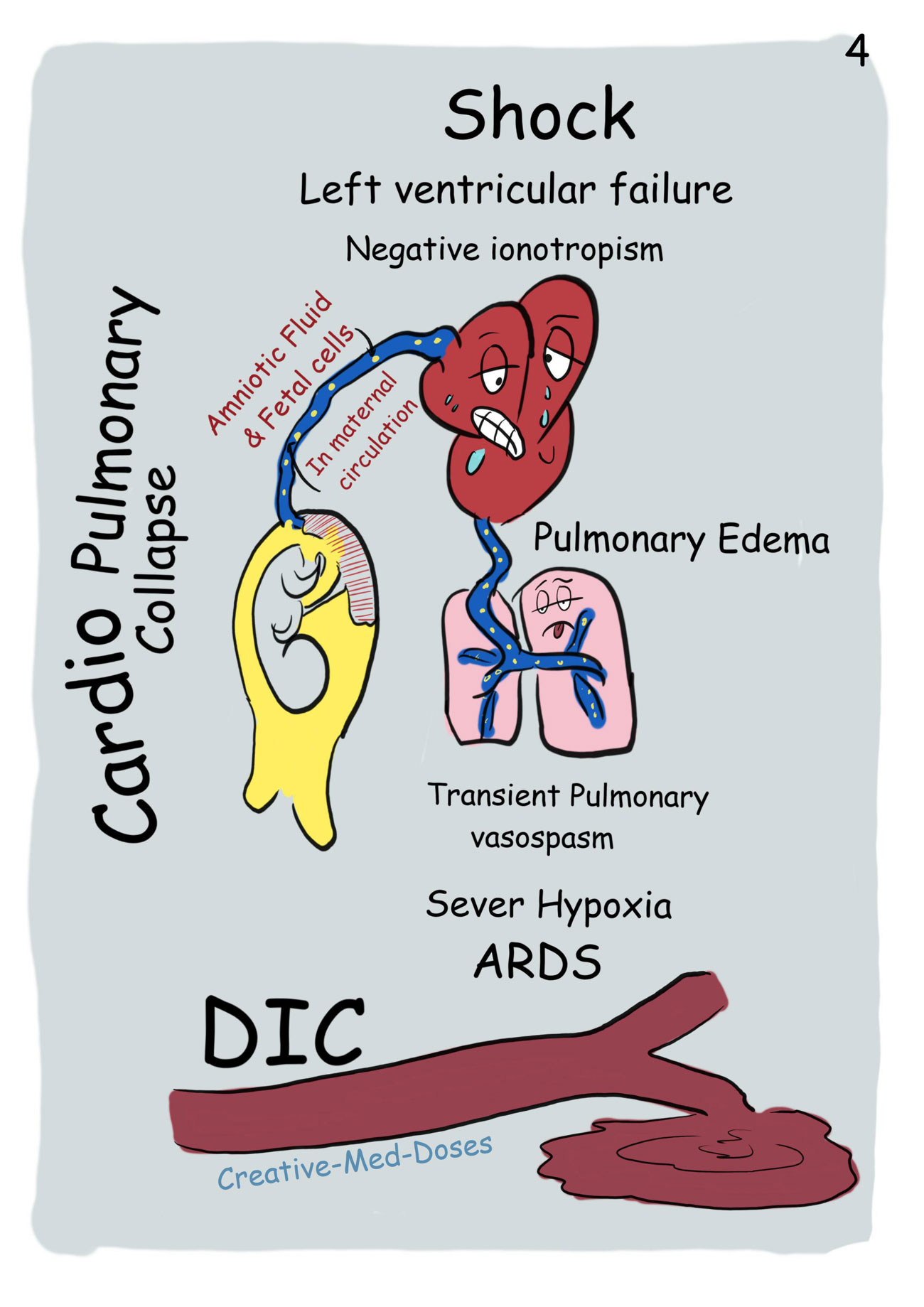
The respiratory reaction begins with a transient pulmonary vasospasm. Vasospasm is caused by amniotic microemboli, which triggers the release of arachidonic acid metabolites and leads to pulmonary hypertension, intrapulmonary shunting, bronchoconstriction, and hypoxia.
The second manifestation is negative inotropism and left ventricular failure causing pulmonary edema and hypotension. It can lead to shock very fast.
The third manifestation includes a neurological response to the respiratory and hemodynamic injury, which may include seizures, confusion, or coma.
To prevent AFE, trauma to the uterus should be avoided during maneuvers such as insertion of a pressure catheter or rupture of membranes. Incision of the placenta during caesarean delivery should also be avoided.
The important factors in the management of AFE are early recognition, prompt resuscitation, and delivery of the fetus. Early recognition of AFE is critical to a successful outcome. Management is mainly supportive and resuscitative.