Addison Disease : primary adrenal insufficiency
Addison disease is a disorder resulting from progressive destruction of the adrenal cortex. Most common cause of chronic adrenal insufficiency/ Addison disease in the Western world (developed world) is the autoimmune adrenalitis, in developing world Tuberculosis is the most common cause.
...
...
Pathogenesis
More than 90% of cases of Addison disease can be attributed to these four
- Autoimmune- most common cause in developed world. Autoimmune adrenalitis is characterized by irregularly shrunken adrenal glands. Adrenals are replaced by collagen and fatty tissue and lymphoid infiltrate is present in the cortex.
- Tuberculosis- most common cause in developing world.
- AIDS- patient of AIDS are prone to infections affecting adrenals and may leads to its destruction.
- Metastatic cancer - Adrenals are common site for metastases in patients with disseminated carcinomas, it destroys adrenal cortex and cause adrenal insufficiency. Carcinomas of the lung and breast are the main cancers which cause metastasis in the adrenals.
Clinical manifestation
In most cases clinical manifestations of adrenocortical insufficiency do not appear until at least 90% of the adrenal cortex has been compromised.
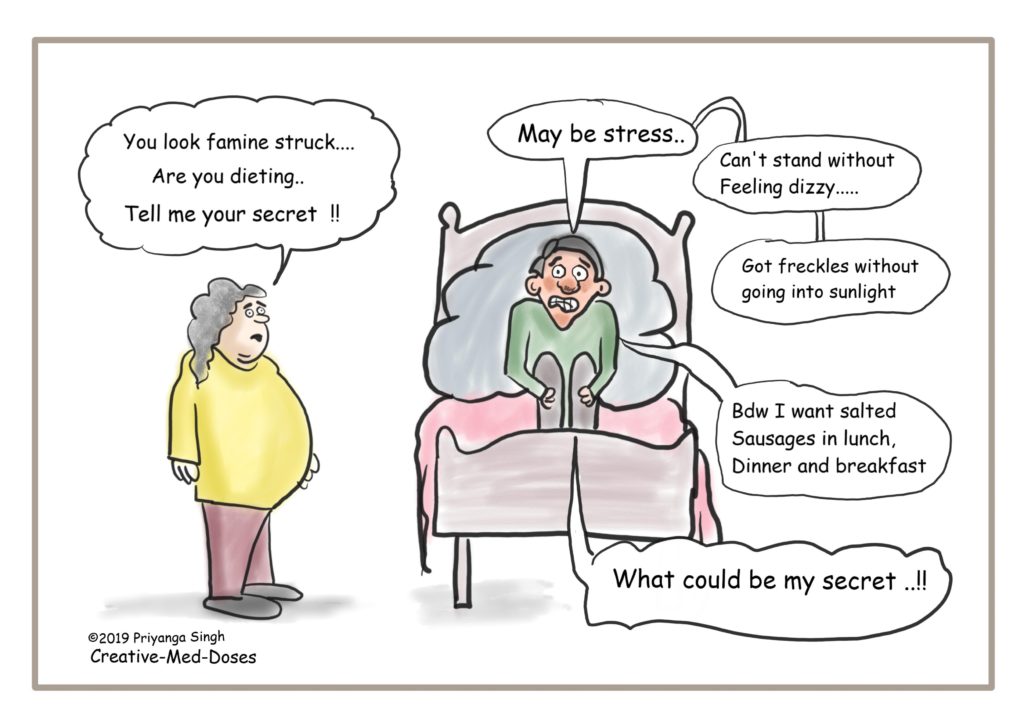
The initial manifestations often include progressive weakness and easy fatigability, which may be dismissed as nonspecific complaints.
Gastrointestinal disturbances are very common and presents as anorexia, nausea, vomiting, weight loss, and occasionally as diarrhea.
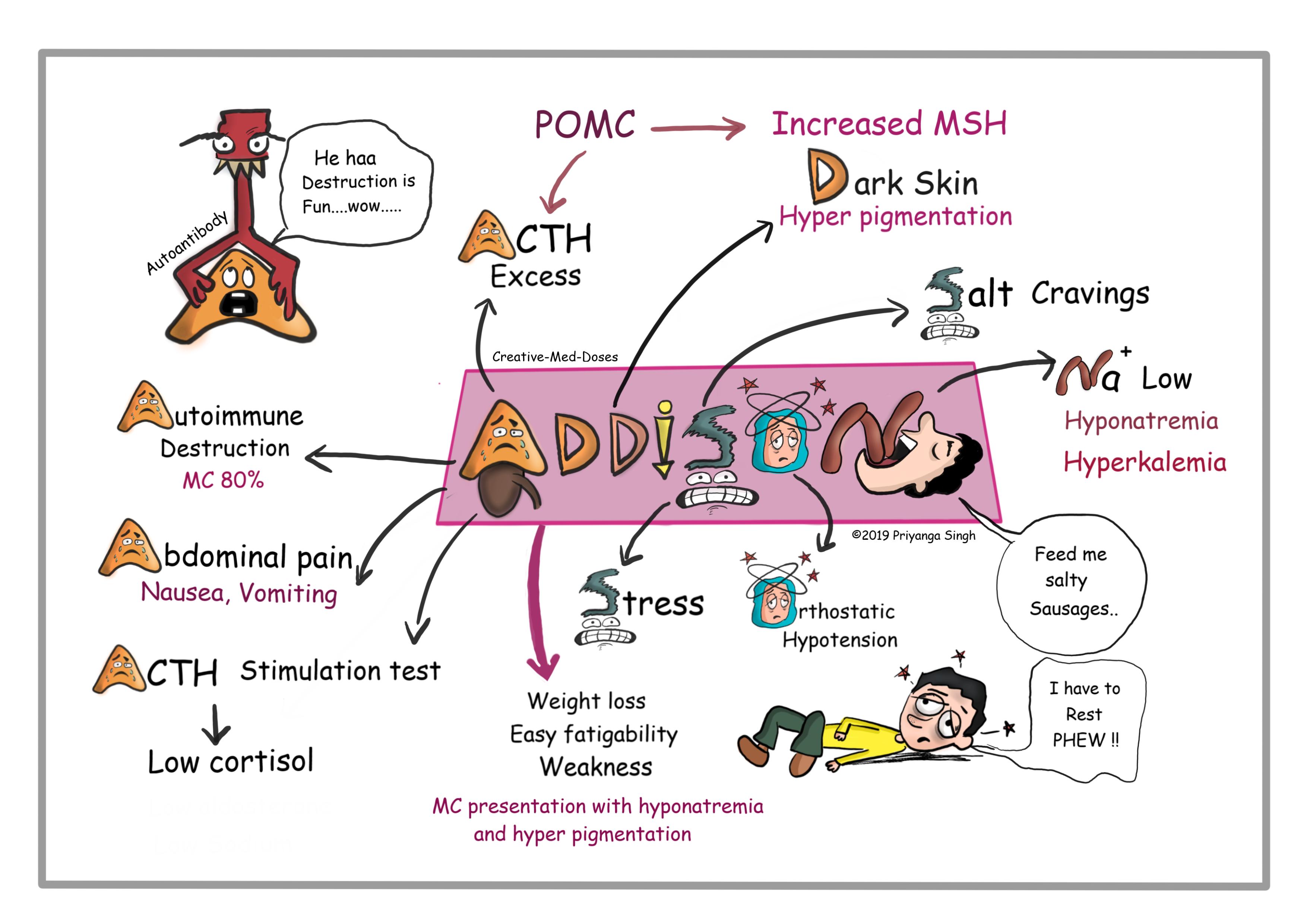
In patients with primary adrenal disease there is increased levels of POMC (pro-opiomelanocortin), which causes increased production of ACTH and MSH. The MSH (melanocyte stimulating hormone) stimulates melanocytes and causes skin hyper pigmentation. Sometimes it starts as freckles. The face, axillae, nipples, areolae, and perineum are particularly common sites of hyperpigmentation.
Decreased mineralocorticoid (aldosterone) activity leads to potassium retention(hyperkalemia) and sodium loss (hyponatremia), loss of sodium causes volume depletion and hypotension. Orthostatic hypotension, dizziness and episodes of fainting are associated with adrenal crisis.
Hypoglycemia occasionally may occur as a result of glucocorticoid deficiency and impaired gluconeogenesis. It is more common in infants and children than adults.
Stresses such as infections, trauma, or surgical procedures may lead to an acute adrenal crisis, manifested by vomiting, abdominal pain, hypotension, coma, and vascular collapse. Death follows rapidly unless corticosteroids are replaced intravenously.
Lab values
- Increased ACTH, with low cortisol and hyponatremia
- Hyperkalemia and low blood glucose
- ACTH stimulation test reveals no rise in cortisol.
Treatment
Replacement therapy
- For glucocorticoids – give Hydrocortisone
- For mineralocorticoids- give fludrocortisone
Case scenario
...
...
A 46-year-old man comes to physician with weakness and easy fatigability. He has orthostatic hypotension and significant weight loss. He also mentions anorexia and stomach cramps. Physical examination reveals freckles and skin hyperpigmentation. Laboratory investigation reveals serum sodium of 126 mEq/L and serum potassium of 6.4 mEq/L. What is most likely diagnosis??
Further reading https://www.sciencedirect.com/science/article/pii/S2214442018300810 and
Revision for today https://creativemeddoses.com/topics-list/listeria-monocytogenes-with-rocket-tail/